Department of Epileptology, University Hospital Bonn, Bonn, Germany.
Department of Nuclear Medicine, University Hospital Bonn, Bonn, Germany.
Epilepsia Open. 2023 Mar;8(1):183-192. doi: 10.1002/epi4.12694. Epub 2023 Jan 30.
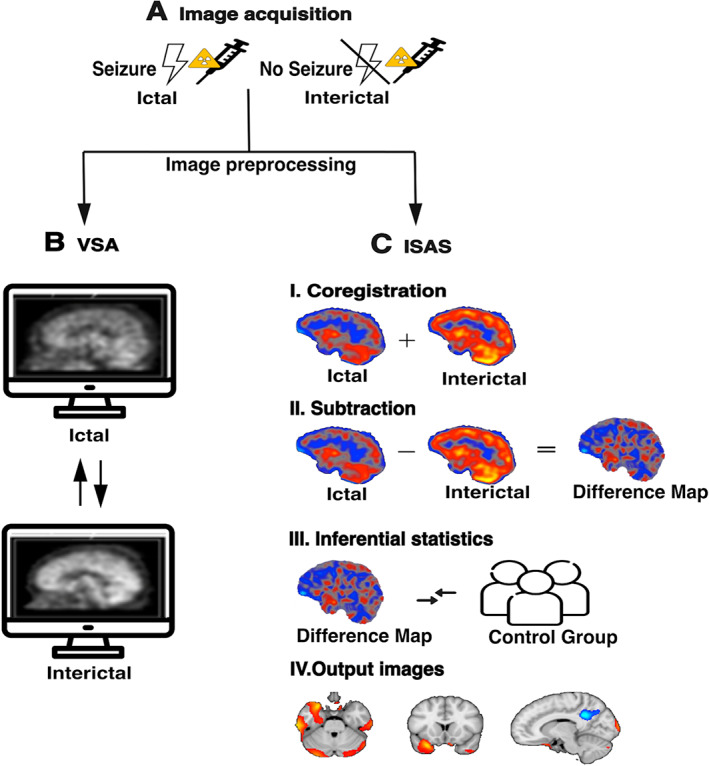
Ictal single photon emission computed tomography (SPECT) can be used as an advanced diagnostic modality to detect the seizure onset zone in the presurgical evaluation of people with epilepsy. In addition to visual assessment (VSA) of ictal and interictal SPECT images, postprocessing methods such as ictal-interictal SPECT analysis using SPM (ISAS) can visualize regional ictal blood flow differences. We aimed to evaluate and differentiate the diagnostic value of VSA and ISAS in the Bonn cohort.
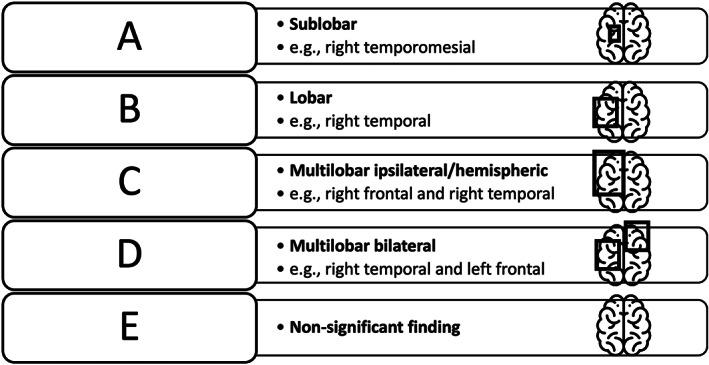
We included 161 people with epilepsy who underwent presurgical evaluation at the University Hospital Bonn between 2008 and 2020 and received ictal and interictal SPECT and ISAS. We retrospectively assigned SPECT findings to one of five categories according to their degree of concordance with the clinical focus hypothesis.
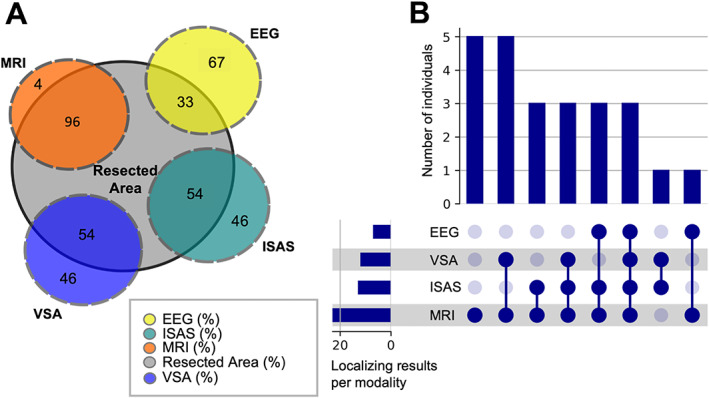
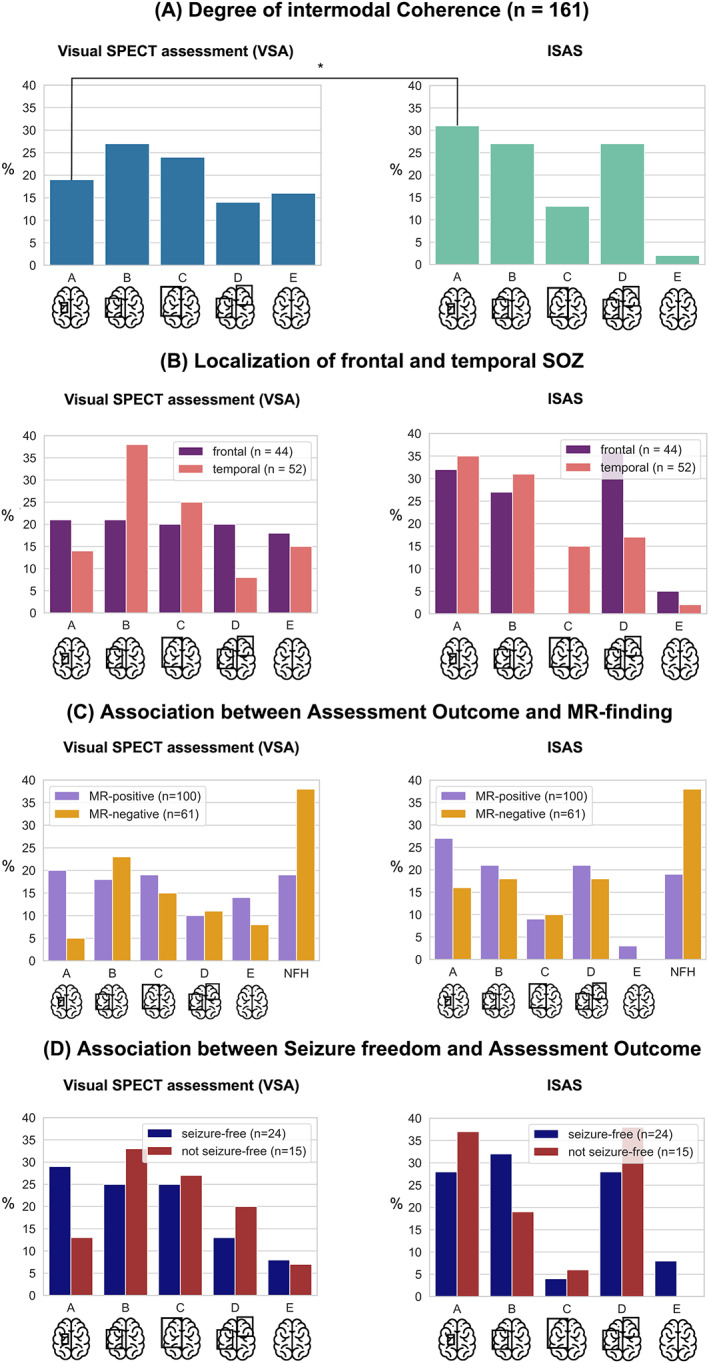
Seizure onset zones could be identified more likely on a sublobar concordance level by ISAS than by VSA (31% vs. 19% of cases; OR = 1.88; 95% Cl [1.04, 3.42]; P = 0.03). Both VSA and ISAS more often localized a temporal seizure onset zone than an extratemporal one. Neither VSA nor ISAS findings were predicted by the latency between seizure onset and tracer injection (P = 0.75). In people who underwent successful epilepsy surgery, VSA and ISAS indicated the correct resection site in 54% of individuals, while MRI and EEG showed the correct resection localization in 96% and 33% of individuals, respectively. It was more likely to become seizure-free after epilepsy surgery if ISAS or VSA had been successful. There was no MR-negative case with successful surgery, indicating that ictal SPECT is more useful for confirmation than for localization.
The results of the most extensive clinical study of ictal SPECT to date allow an assessment of the diagnostic value of this elaborate examination and emphasize the importance of postprocessing routines.
发作期单光子发射计算机断层扫描(SPECT)可用作先进的诊断手段,以检测癫痫患者术前评估中的致痫区。除了发作期和发作间期 SPECT 图像的视觉评估(VSA)之外,还可以使用 SPM(ISAS)对发作期-发作间期 SPECT 分析等后处理方法来可视化区域发作期血流差异。我们旨在评估和区分 Bonn 队列中 VSA 和 ISAS 的诊断价值。
我们纳入了 2008 年至 2020 年期间在波恩大学医院接受术前评估的 161 名癫痫患者,他们接受了发作期和发作间期 SPECT 和 ISAS。我们回顾性地根据 SPECT 发现与临床焦点假说的一致性程度,将 SPECT 结果分为五个类别之一。
ISAS 比 VSA 更有可能在亚叶水平上确定致痫区(31%与 19%的病例;OR=1.88;95%CI[1.04,3.42];P=0.03)。VSA 和 ISAS 都更常定位颞叶发作起始区而非颞外发作起始区。VSA 和 ISAS 结果均不受发作起始与示踪剂注射之间潜伏期的影响(P=0.75)。在成功接受癫痫手术的患者中,VSA 和 ISAS 在 54%的个体中指示了正确的切除部位,而 MRI 和 EEG 分别在 96%和 33%的个体中显示了正确的切除定位。如果 ISAS 或 VSA 成功,术后成为无癫痫发作的可能性更大。没有 MRI 阴性但手术成功的病例,这表明发作期 SPECT 更有助于确认而非定位。
迄今为止最广泛的发作期 SPECT 临床研究结果可评估该精细检查的诊断价值,并强调后处理程序的重要性。