Wang Joanna Nan, Olsen Niels Thue, Taraldsen Ida Arentz, Mogelvang Rasmus
Department of Cardiology, The Heart Centre, Copenhagen University Hospital - Rigshospitalet, Copenhagen, Denmark.
Copenhagen City Heart Study, Copenhagen University Hospital - Bispebjerg and Frederiksberg Hospital, Frederiksberg, Denmark.
Front Cardiovasc Med. 2023 Jan 4;9:1040647. doi: 10.3389/fcvm.2022.1040647. eCollection 2022.
Tissue Doppler imaging (TDI) is a sensitive marker of impaired cardiac function and different phases of the TDI curve carry different prognostic information. It is not known how continuous TDI curves change with age in normal subjects, and whether these changes differ from changes seen in individuals at risk of future cardiac events.
A total of 1,763 individuals from the general population were examined with color TDI at the septal and lateral mitral sites. A low-risk group was defined as without cardiac risk factors (hypertension, diabetes or ischemic heart disease) at baseline and without any cardiac events (cardiovascular death or admission due to either heart failure or acute myocardial infarction) during 10-years follow-up. All TDI curves were corrected for heart rate, and whole-cycle analysis of age-related changes to TDI velocities was performed in both low-risk ( = 881) and high-risk individuals ( = 882).
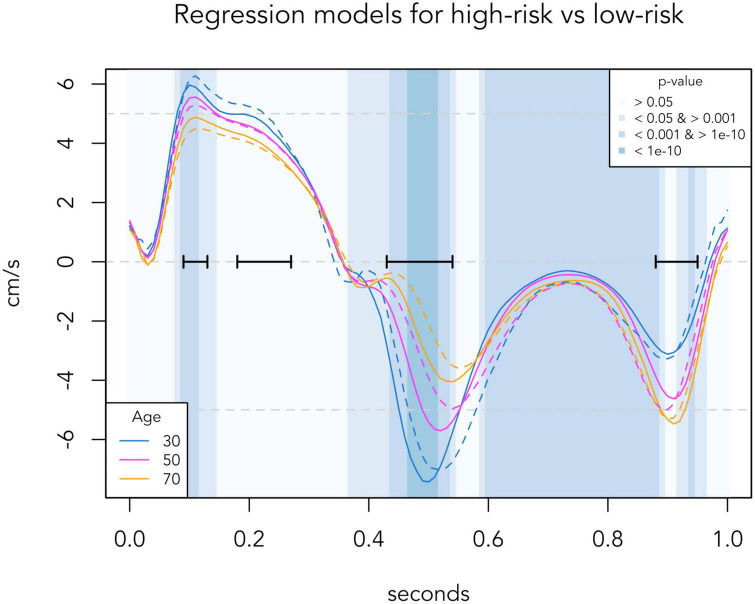
In the low-risk population, four phases where myocardial velocity differed most ( < 10) according to age were identified [in a standardized cardiac cycle of 1 second (s)]: Systolic peak (0.09-0.13 s), systolic plateau (0.18-0.27 s), early diastole (0.43-0.54 s) and late diastole (0.88-0.95 s). With increasing age, systolic velocities decreased, early diastolic velocities decreased and had delayed peak, and late diastolic velocities increased until age 70 and then stopped increasing. In the high-risk population, comparison to corresponding age groups of the low-risk population showed: Lower early diastolic velocities in 20-40-year-olds; higher late diastolic velocities and lower peak systolic velocities in 40-60-year-olds; further decreased systolic velocities including the systolic plateau and decreased late diastolic velocities in 60-year-olds. The time segments around the systolic peak ( = 0.002) and early diastole ( < 0.001) differed significantly between the high-risk and low-risk population, thus making it possible to use the individual age gap between a TDI-derived biological age and the real chronological age as a tool to discriminate high-risk individuals from low-risk individuals.
We found that individuals with cardiac risk factors display findings compatible with an accelerated aging of the heart and thus propose TDI-derived biological age as a tool to identify high-risk patients.
组织多普勒成像(TDI)是心脏功能受损的敏感标志物,TDI曲线的不同阶段携带不同的预后信息。目前尚不清楚正常受试者的连续TDI曲线如何随年龄变化,以及这些变化是否与未来有心脏事件风险的个体所观察到的变化不同。
对来自普通人群的1763名个体在二尖瓣间隔和侧壁部位进行彩色TDI检查。低风险组定义为基线时无心脏危险因素(高血压、糖尿病或缺血性心脏病)且在10年随访期间无任何心脏事件(心血管死亡或因心力衰竭或急性心肌梗死入院)。所有TDI曲线均进行心率校正,并在低风险(n = 881)和高风险个体(n = 882)中对TDI速度的年龄相关变化进行全周期分析。
在低风险人群中,根据年龄确定了心肌速度差异最大(P < 0.01)的四个阶段[在1秒(s)的标准化心动周期中]:收缩期峰值(0.09 - 0.13 s)、收缩期平台期(0.18 - 0.27 s)、舒张早期(0.43 - 0.54 s)和舒张晚期(0.88 - 0.95 s)。随着年龄的增长,收缩期速度降低,舒张早期速度降低且峰值延迟,舒张晚期速度在70岁之前增加,之后停止增加。在高风险人群中,与低风险人群的相应年龄组相比显示:20 - 40岁人群舒张早期速度较低;40 - 60岁人群舒张晚期速度较高且收缩期峰值速度较低;60岁人群收缩期速度进一步降低,包括收缩期平台期,舒张晚期速度降低。收缩期峰值(P = 0.002)和舒张早期(P < 0.001)周围的时间段在高风险和低风险人群之间有显著差异,因此可以将TDI衍生的生物学年龄与实际年龄之间的个体年龄差距作为区分高风险个体和低风险个体的工具。
我们发现有心脏危险因素的个体表现出与心脏加速老化相符的结果,因此提出将TDI衍生的生物学年龄作为识别高风险患者的工具。