Collister David, Farrar Mark, Farrar Lesha, Brown Paul, Booth Michelle, Firth Tracy, Mahr Alfred, Zeng Linan, Little Mark A, Mustafa Reem A, Fussner Lynn A, Meara Alexa, Guyatt Gordon, Jayne David, Merkel Peter A, Walsh Michael
Division of Nephrology, Department of Medicine, University of Alberta, Edmonton, Alberta, Canada.
Population Health Research Institute, Hamilton, Ontario, Canada.
Kidney Med. 2022 Dec 24;5(3):100595. doi: 10.1016/j.xkme.2022.100595. eCollection 2023 Mar.
RATIONALE & OBJECTIVE: We sought to elicit patient preferences regarding the use of plasma exchange in antineutrophil cytoplasmic antibody-associated vasculitis (AAV) and its tradeoffs of risk of kidney failure and risk of serious infection.
Patient survey.
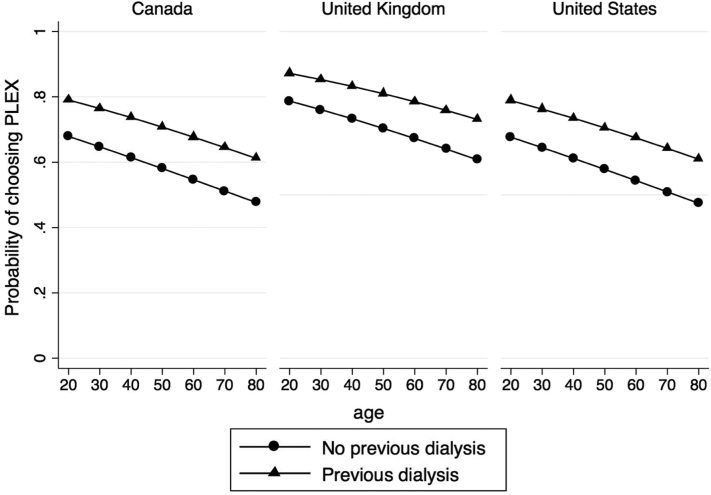
SETTING & PARTICIPANTS: The online survey was circulated to adults with AAV via kidney and vasculitis networks in Canada, the United Kingdom, and the United States.
Respondents reviewed the estimated 1-year risks of kidney failure and serious infection in AAV with and without plasma exchange across 5 serum creatinine categories (150, 250, 350, 450, and 600 μmol/L). For each scenario, participants indicated whether or not they would choose plasma exchange.
Responses were assessed with multilevel multivariable logistic regression models to identify predictors of respondent choice regarding treatment with plasma exchange.
The 470 respondents from the 13 countries (United States 61.7%, United Kingdom 20.0%, Canada 13.8%, and other countries 4.5%) had a mean age of 58.6 (SD 14.3) years, 70.2% women. Respondents were more likely to choose plasma exchange in scenarios at high risk of kidney failure and serious infection (creatinine level of 350 or 450 μmol/L) compared with lower risk scenarios or the highest risk scenario. However, 145 (30.9%) chose plasma exchange across all scenarios, whereas 80 (17.0%) declined plasma exchange across all scenarios. Respondents from the United Kingdom (OR, 2.61; 95% CI, 1.09-6.22) who received previous dialysis (OR, 2.70; 95% CI, 1.12-6.52) or received previous plasma exchange (OR, 5.62; 95% CI, 2.72-11.61) were more likely to choose plasma exchange, whereas older respondents (OR, 0.98; 95% CI, 0.96-0.99 per 1 year increase) were less likely.
Unclear generalizability to non-English-speaking, older, and less health literate adults, possible responder bias, survivor bias, lack of individualized risk assessments for kidney failure, and serious infection.
Patients with AAV do not express a consistent choice for plasma exchange, which highlights the need for shared decision making.
我们旨在了解患者对于在抗中性粒细胞胞浆抗体相关性血管炎(AAV)中使用血浆置换的偏好,以及其在肾衰竭风险和严重感染风险之间的权衡。
患者调查。
通过加拿大、英国和美国的肾脏与血管炎网络,向患有AAV的成年人发放在线调查问卷。
受访者查看了在5种血清肌酐类别(150、250、350、450和600μmol/L)下,有或无血浆置换的AAV患者中估计的1年肾衰竭和严重感染风险。对于每种情况,参与者表明他们是否会选择血浆置换。
使用多水平多变量逻辑回归模型评估回答,以确定受访者选择血浆置换治疗的预测因素。
来自13个国家的470名受访者(美国61.7%,英国20.0%,加拿大13.8%,其他国家4.5%)的平均年龄为58.6(标准差14.3)岁,女性占70.2%。与低风险情况或最高风险情况相比,受访者在肾衰竭和严重感染高风险情况(肌酐水平为350或450μmol/L)下更有可能选择血浆置换。然而,145名(30.9%)受访者在所有情况下都选择血浆置换,而80名(17.0%)受访者在所有情况下都拒绝血浆置换。来自英国的受访者(比值比,2.61;95%置信区间,1.09 - 6.22)、曾接受透析的受访者(比值比,2.70;95%置信区间,1.12 - 6.52)或曾接受血浆置换的受访者(比值比,5.62;95%置信区间,2.72 - 11.61)更有可能选择血浆置换,而年龄较大的受访者(比值比,0.98;95%置信区间,每增加1岁为0.96 - 0.99)则不太可能选择。
对于非英语、年龄较大和健康素养较低的成年人,普遍适用性尚不清楚,可能存在应答者偏差、幸存者偏差,缺乏针对肾衰竭和严重感染的个体化风险评估。
AAV患者对于血浆置换并未表现出一致的选择,这凸显了共同决策的必要性。