Shahzad Muhammad Asim, Aziz Khawaja Talha, Korbet Stephen
Division of Nephrology, RUSH University Medical Center, Chicago, IL, USA.
Khyber Teaching Hospital, Peshawar, Pakistan.
Can J Kidney Health Dis. 2023 Jan 18;10:20543581221150554. doi: 10.1177/20543581221150554. eCollection 2023.
sp. are the most common causes of culture-negative infective endocarditis (IE) cases in the United States. Although, infection-related glomerulonephritis can frequently mimic primary vasculitis due to pauci-immune pattern, majority of previously reported cases of -associated glomerulonephritis have immune-complex deposits on immunofluorescence. We present a rare case of IE-related pauci-immune necrotizing glomerulonephritis. Timely recognition of this atypical presentation led to appropriately directed medical therapy.
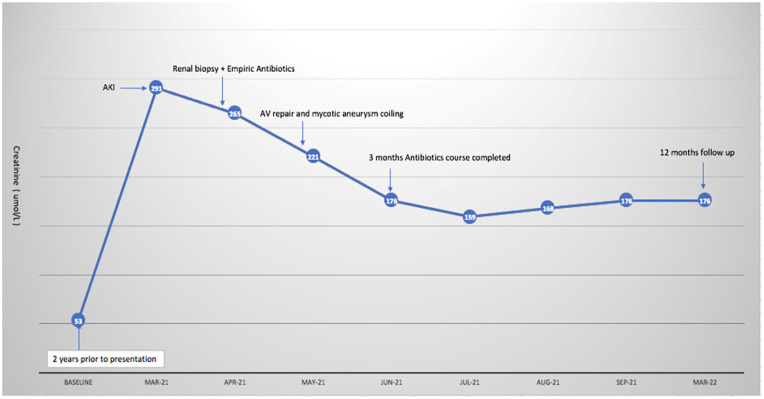
A 33-year-old Caucasian male with a history of human immunodeficiency virus (HIV) on highly active antiretroviral therapy (HAART), alcohol abuse, previous subarachnoid hemorrhage (SAH), and recent wisdom tooth extraction (on amoxicillin) was transferred from an outside hospital for further evaluation of severe headache. He was diagnosed with an SAH and right anterior cerebral artery mycotic aneurysm. The serum creatinine at the outside hospital was 292 umol/L (3.3 mg/dL) with a previously normal baseline around 2 years ago. The serum creatinine at our institution was 256 umol/L (3.0 mg/dL). The urinalysis demonstrated +100 protein, +3 blood and 29 red blood cells/high power field. The urine protein creatinine ratio (UPC) was 1.7 g/g. Serologic evaluation was positive for a low C4 10.2 mg/dL, elevated rheumatoid factor 40 IU/mL and an elevated proteinase 3 (PR-3) antineutrophilic cytoplasmic antibodies (ANCA Ab) 4.0 U/mL. A transesophageal echocardiogram (TEE) showed echo densities on both mitral and aortic valve. Blood cultures were negative. Further serologic evaluation was positive for IgG titer of 1:2560 (normal <1:320) with a negative IgM titer.
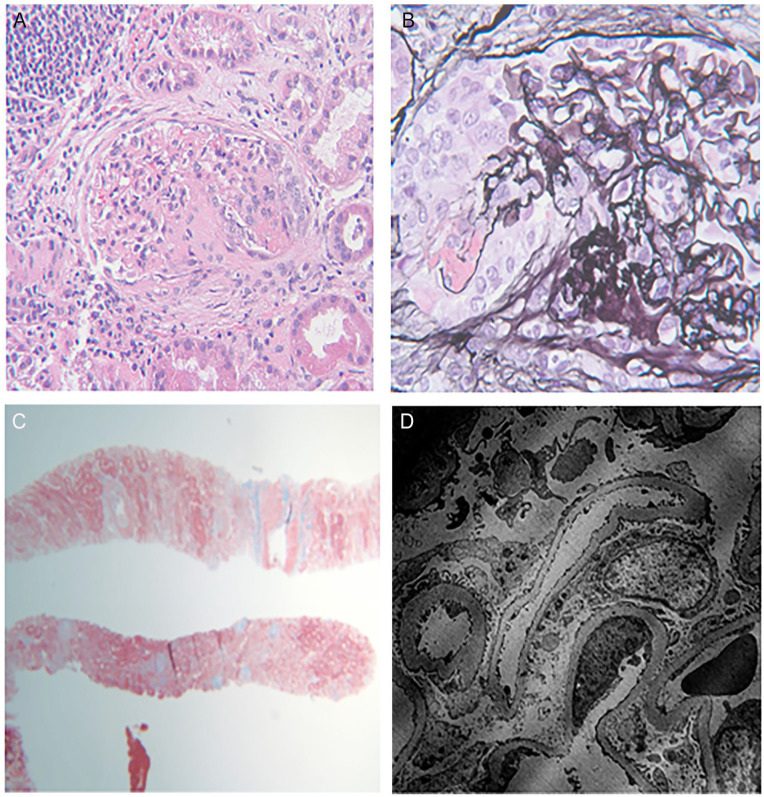
A percutaneous kidney biopsy revealed pauci-immune necrotizing glomerulonephritis, with 14/16 glomeruli globally sclerotic, and 2 glomeruli with active segmental necrotizing lesions. There was no evidence of immune-complex deposition on immunofluorescence or electron microscopy. Clinical findings were consistent with IE associated mycotic aneurysm and necrotizing glomerulonephritis.
Empiric treatment for an active glomerulonephritis with immunosuppressive agents was deferred on admission, given concern for an underlying infectious process and mycotic aneurysms in an HIV-positive patient. He received antibiotic treatment with doxycycline and ceftriaxone with gentamicin for synergy. Despite this, the mitral and aortic valve regurgitation worsened, and he developed congestive heart failure requiring aortic valve replacement and mitral valve repair. The explanted aortic valve was positive for by polymerase chain reaction (PCR) confirming the diagnosis of IE.
Immunosuppression was deferred due to timely identification of an atypical presentation of -associated ANCA antibodies-positive, pauci-immune necrotizing glomerulonephritis. A course of antibiotic treatment resulted in improved renal functions along with undetectable and PR3 Ab titers. The serum creatinine decreased to 176 umol/L (2 mg/dL) and remained stable 12 months after discharge.
IE should be suspected in patients with pauci-immune necrotizing glomerulonephritis and culture-negative IE. This is imperative for optimal decision making in the management of such patients. Having high clinical suspicion can avoid unnecessary and potentially deleterious use of immunosuppressive agents.
在美国,[病原体名称未给出]是血培养阴性感染性心内膜炎(IE)病例最常见的病因。尽管感染相关的肾小球肾炎由于寡免疫模式常可模仿原发性血管炎,但先前报道的大多数[病原体名称未给出]相关肾小球肾炎病例在免疫荧光检查时有免疫复合物沉积。我们报告一例罕见的IE相关寡免疫坏死性肾小球肾炎病例。及时识别这种非典型表现可指导进行适当的药物治疗。
一名33岁的白人男性,有人类免疫缺陷病毒(HIV)病史,正在接受高效抗逆转录病毒治疗(HAART),有酗酒史、既往蛛网膜下腔出血(SAH)史,近期拔除智齿(服用阿莫西林),因严重头痛从外院转入进一步评估。他被诊断为SAH和右大脑前动脉霉菌性动脉瘤。外院血清肌酐为292 μmol/L(3.3 mg/dL),约2年前基线水平正常。我院血清肌酐为256 μmol/L(3.0 mg/dL)。尿液分析显示尿蛋白+++、血尿+++,高倍视野下有29个红细胞。尿蛋白肌酐比值(UPC)为1.7 g/g。血清学评估显示C4降低至10.2 mg/dL、类风湿因子升高至40 IU/mL、蛋白酶3(PR-3)抗中性粒细胞胞浆抗体(ANCA Ab)升高至4.0 U/mL。经食管超声心动图(TEE)显示二尖瓣和主动脉瓣有回声增强。血培养阴性。进一步血清学评估显示IgG滴度为1:2560(正常<1:320),IgM滴度阴性。
经皮肾活检显示寡免疫坏死性肾小球肾炎,16个肾小球中有14个全球硬化,2个肾小球有活动性节段坏死性病变。免疫荧光或电子显微镜检查未发现免疫复合物沉积证据。临床发现与IE相关的霉菌性动脉瘤和坏死性肾小球肾炎一致。
鉴于对一名HIV阳性患者潜在感染过程和霉菌性动脉瘤的担忧,入院时暂未对活动性肾小球肾炎使用免疫抑制剂进行经验性治疗。他接受了强力霉素、头孢曲松联合庆大霉素的抗生素治疗以增强协同作用。尽管如此,二尖瓣和主动脉瓣反流仍加重,他发展为充血性心力衰竭,需要进行主动脉瓣置换和二尖瓣修复。经聚合酶链反应(PCR)检测,切除的主动脉瓣[病原体名称未给出]呈阳性,确诊为IE。
由于及时识别了与[病原体名称未给出]相关的ANCA抗体阳性寡免疫坏死性肾小球肾炎的非典型表现,暂未进行免疫抑制治疗。一个疗程的抗生素治疗使肾功能改善,[病原体名称未给出]和PR3 Ab滴度检测不到。血清肌酐降至176 μmol/L(2 mg/dL),出院12个月后保持稳定。
对于寡免疫坏死性肾小球肾炎和血培养阴性IE患者应怀疑IE。这对于此类患者管理的最佳决策至关重要。高度的临床怀疑可避免不必要且可能有害的免疫抑制剂使用。