Department of Radiology, Addenbrooke's Hospital, Cambridge University Hospitals NHS Foundation Trust, Hills Rd, Cambridge, CB2 0QQ, UK.
Department of Cardiology, Royal Papworth Hospital NHS Foundation Trust, Papworth Rd, Trumpington, Cambridge, CB2 0AY, UK.
Eur Radiol. 2023 Jul;33(7):4723-4733. doi: 10.1007/s00330-023-09428-z. Epub 2023 Jan 27.
To assess coronary artery calcification (CAC) on non-contrast non-ECG-gated CT thorax (NC-NECG-CTT) and to evaluate its correlation with short-term risk of cardiovascular disease (CVD) events and death.
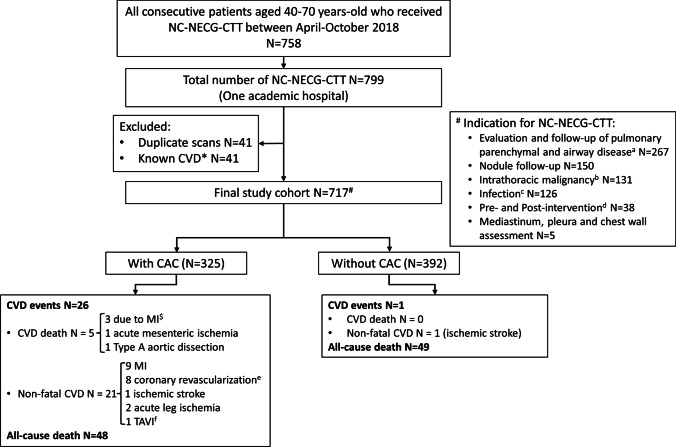
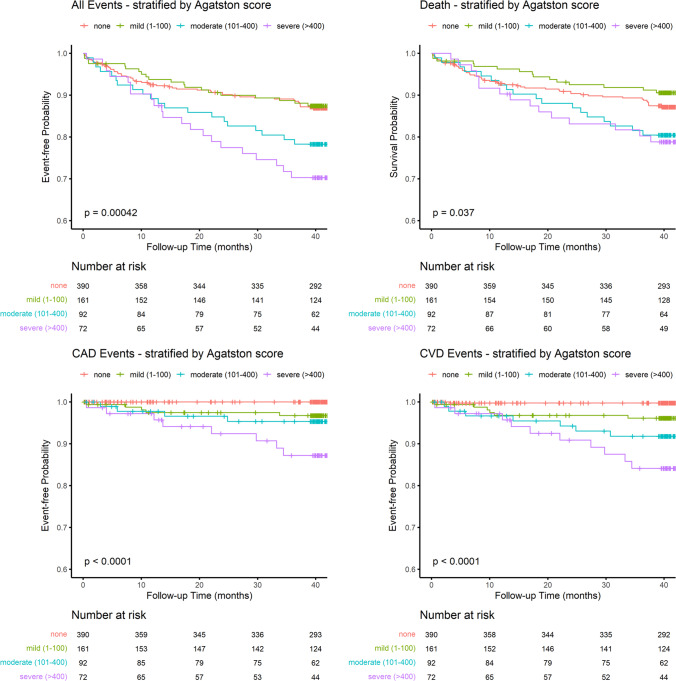
Single-institution retrospective study including all patients 40-70 years old who underwent NC-NECG-CTT over a period of 6 months. Individuals with known CVD were excluded. The presence of CAC was assessed and quantified by the Agatston score (CACS). CAC severity was defined as mild (< 100), moderate (100-400), or severe (> 400). CVD events (including CVD death, myocardial infarction, revascularisation procedures, ischaemic stroke, acute peripheral atherosclerotic ischaemia), and all-cause mortality over a median of 3.5 years were recorded. Cox proportional-hazards regression modelling was performed including CACS, age, gender and CVD risk factors (smoking, hypertension, diabetes mellitus, dyslipidaemia, and family history of CVD).
Of the total 717 eligible cases, 325 (45%) had CAC. In patients without CAC, there was only one CVD event, compared to 26 CVD events including 5 deaths in patients with CAC. The presence and severity of CAC correlated with CVD events (p < 0.001). A CACS > 100 was significantly associated with both CVD events, hazard ratio (HR) 5.74, 95% confidence interval: 2.19-15.02; p < 0.001, and all-cause mortality, HR 1.7, 95% CI: 1.08-2.66; p = 0.02. Ever-smokers with CAC had a significantly higher risk for all-cause mortality compared to never-smokers (p = 0.03), but smoking status was not an independent predictor for CVD events in any subgroup category of CAC severity.
The presence and severity of CAC assessed on NC-NECG-CTT correlates with short-term cardiovascular events and death.
• Patients aged 40-70 years old without known CVD but with CAC on NC-NECG-CTT have a higher risk of CVD events compared to those without CAC. • CAC (Agatston) score above 100 confers a 5.7-fold increase in the risk of short-term CVD events in these patients. • The presence and severity of CAC on NC-NECG-CTT may have prognostic and therapeutic implications.
评估非对比非心电图门控胸部 CT(NC-NECG-CTT)上的冠状动脉钙化(CAC),并评估其与短期心血管疾病(CVD)事件和死亡风险的相关性。
这是一项单中心回顾性研究,纳入了在 6 个月期间接受 NC-NECG-CTT 的所有 40-70 岁患者。排除已知 CVD 的个体。通过 Agatston 评分(CACS)评估和量化 CAC 的存在和严重程度。CAC 严重程度定义为轻度(<100)、中度(100-400)或重度(>400)。记录中位随访 3.5 年内的 CVD 事件(包括 CVD 死亡、心肌梗死、血运重建术、缺血性卒中和急性外周动脉粥样硬化性缺血)和全因死亡率。使用 Cox 比例风险回归模型包括 CACS、年龄、性别和 CVD 危险因素(吸烟、高血压、糖尿病、血脂异常和 CVD 家族史)。
在总共 717 例合格病例中,325 例(45%)有 CAC。在没有 CAC 的患者中,只有 1 例 CVD 事件,而在有 CAC 的患者中,有 26 例 CVD 事件,包括 5 例死亡。CAC 的存在和严重程度与 CVD 事件相关(p<0.001)。CACS>100 与 CVD 事件显著相关,风险比(HR)为 5.74,95%置信区间:2.19-15.02;p<0.001,以及全因死亡率,HR 为 1.7,95%CI:1.08-2.66;p=0.02。有 CAC 的吸烟者全因死亡率明显高于无 CAC 的吸烟者(p=0.03),但在 CAC 严重程度的任何亚组类别中,吸烟状况均不是 CVD 事件的独立预测因素。
NC-NECG-CTT 上 CAC 的存在和严重程度与短期心血管事件和死亡相关。
年龄在 40-70 岁之间、无已知 CVD 但在 NC-NECG-CTT 上有 CAC 的患者与无 CAC 的患者相比,CVD 事件的风险更高。
在这些患者中,CAC(Agatston)评分>100 可使短期 CVD 事件的风险增加 5.7 倍。
NC-NECG-CTT 上 CAC 的存在和严重程度可能具有预后和治疗意义。