Department of Pediatrics, Children's Mercy Kansas City, Kansas City, MO; Department of Pathology and Laboratory Medicine, Children's Mercy Kansas City, Kansas City, MO; Division of Clinical Genetics, Department of Pediatrics, Children's Mercy Kansas City, Kansas City, MO.
Department of Pediatrics, Children's Mercy Kansas City, Kansas City, MO; Department of Pathology and Laboratory Medicine, Children's Mercy Kansas City, Kansas City, MO.
Genet Med. 2023 May;25(5):100020. doi: 10.1016/j.gim.2023.100020. Epub 2023 Jan 28.
This study aimed to assess the amount and types of clinical genetic testing denied by insurance and the rate of diagnostic and candidate genetic findings identified through research in patients who faced insurance denials.
Analysis consisted of review of insurance denials in 801 patients enrolled in a pediatric genomic research repository with either no previous genetic testing or previous negative genetic testing result identified through cross-referencing with insurance prior-authorizations in patient medical records. Patients and denials were also categorized by type of insurance coverage. Diagnostic findings and candidate genetic findings in these groups were determined through review of our internal variant database and patient charts.
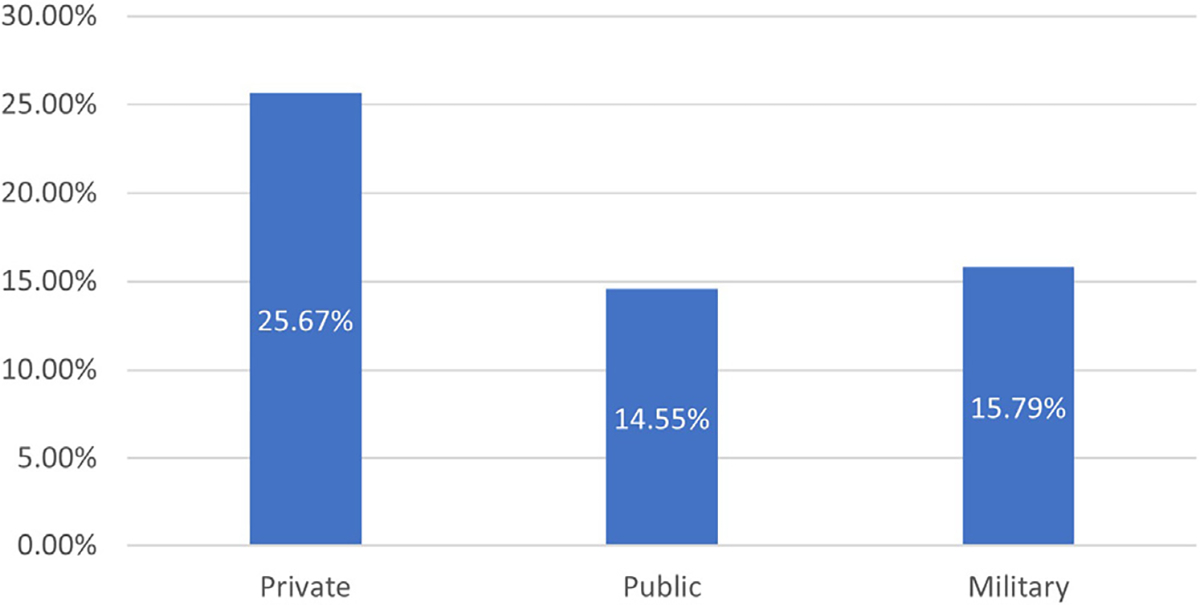
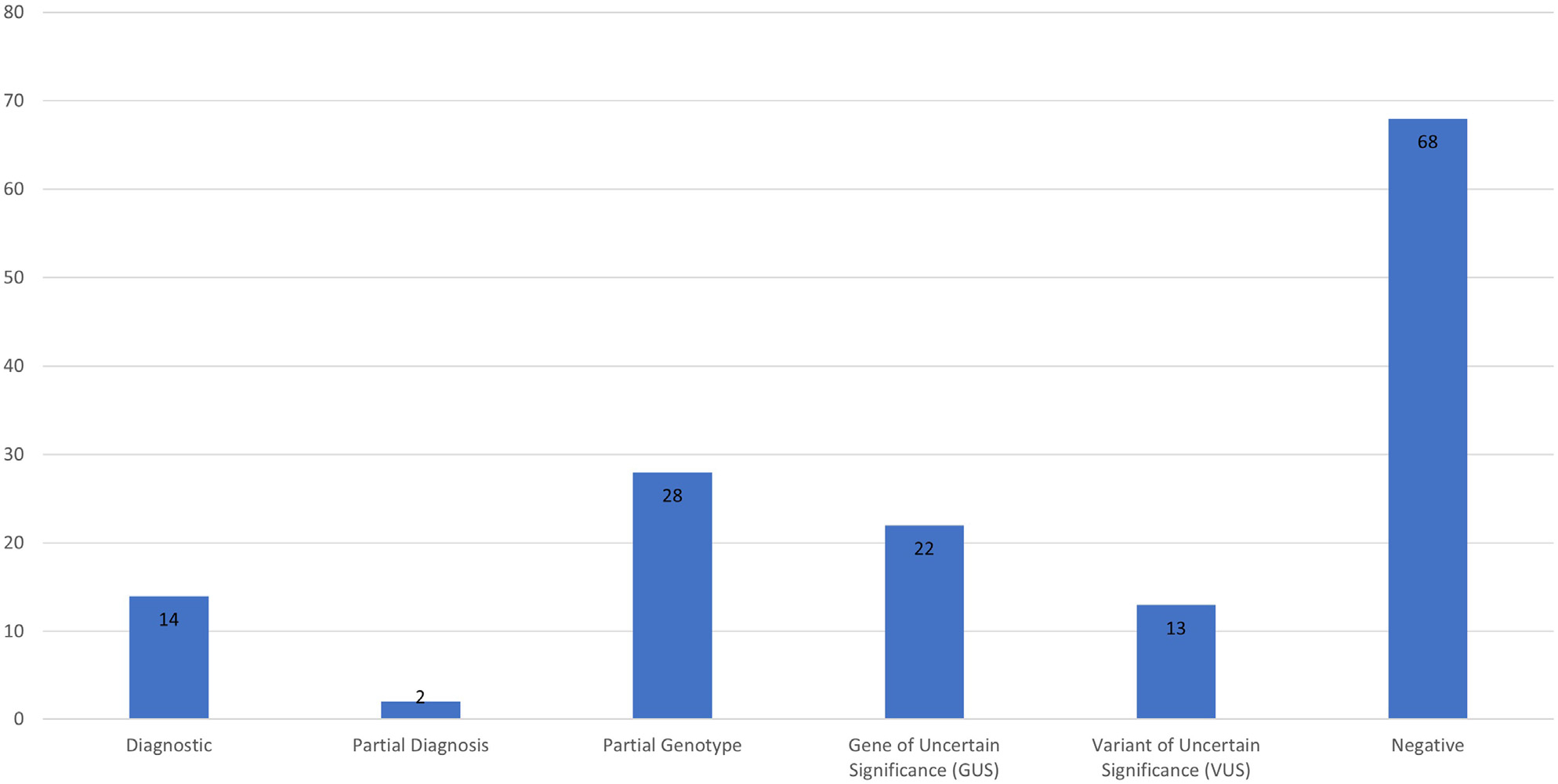
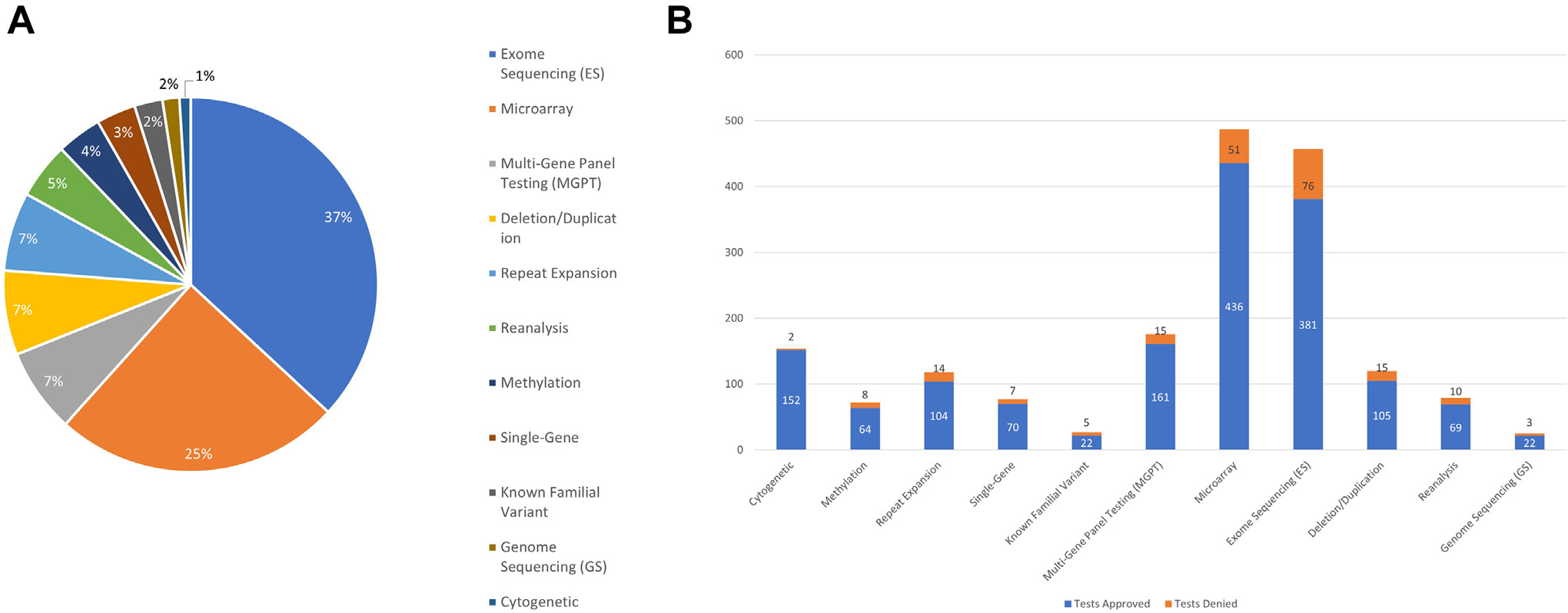
Of the 801 patients analyzed, 147 had insurance prior-authorization denials on record (18.3%). Exome sequencing and microarray were the most frequently denied genetic tests. Private insurance was significantly more likely to deny testing than public insurance (odds ratio = 2.03 [95% CI = 1.38-2.99] P = .0003). Of the 147 patients with insurance denials, 53.7% had at least 1 diagnostic or candidate finding and 10.9% specifically had a clinically diagnostic finding. Fifty percent of patients with clinically diagnostic results had immediate medical management changes (5.4% of all patients experiencing denials).
Many patients face a major barrier to genetic testing in the form of lack of insurance coverage. A number of these patients have clinically diagnostic findings with medical management implications that would not have been identified without access to research testing. These findings support re-evaluation of insurance carriers' coverage policies.
本研究旨在评估保险拒赔的临床基因检测数量和类型,以及在面临保险拒赔的患者中,通过研究确定的诊断和候选基因发现的比例。
分析包括对 801 名入组儿科基因组研究存储库的患者的保险拒赔进行审查,这些患者要么没有先前的基因检测,要么通过与患者病历中的保险预授权交叉引用确定先前的阴性基因检测结果。还按保险类型对患者和拒赔进行了分类。通过审查我们的内部变异数据库和患者图表,确定了这些组中的诊断发现和候选基因发现。
在分析的 801 名患者中,有 147 名患者的保险预授权拒赔记录(18.3%)。外显子组测序和微阵列是最常被拒绝的基因检测。私人保险比公共保险更有可能拒绝检测(优势比=2.03[95%CI=1.38-2.99]P=0.0003)。在 147 名有保险拒赔的患者中,53.7%至少有 1 个诊断或候选发现,10.9%有明确的临床诊断发现。有临床诊断结果的患者中有 50%(所有拒赔患者的 5.4%)立即进行了医疗管理变更。
许多患者面临缺乏保险覆盖的主要基因检测障碍。这些患者中有许多具有临床诊断意义的发现,如果没有研究检测的机会,这些发现将无法被识别。这些发现支持重新评估保险公司的承保政策。