Kim Nina, Estrada Joaquin, Chow Isabella, Ruseva Aleksandrina, Ramasamy Abhilasha, Burudpakdee Chakkarin, Blanchette Christopher M
Novo Nordisk, Inc, Plainsboro, NJ, USA.
IQVIA, Inc, San Francisco, CA, USA.
Clinicoecon Outcomes Res. 2023 Jan 26;15:51-62. doi: 10.2147/CEOR.S392276. eCollection 2023.
To demonstrate a need for improved health insurance coverage for anti-obesity medications (AOMs) by comparing clinical and economic benefits of obesity treatments to covered medications for selected therapeutic areas.
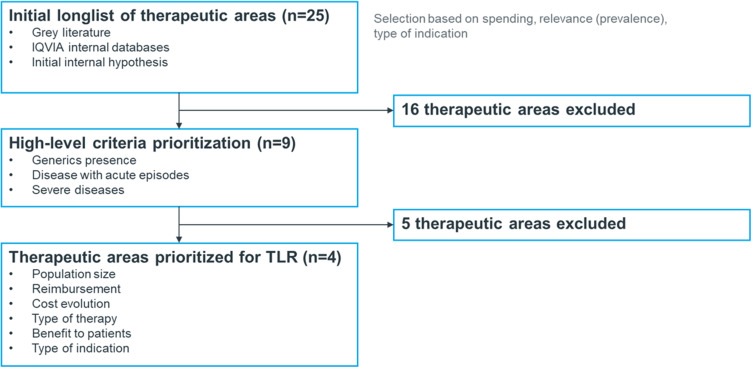
Using a grey literature search, we identified and prioritized therapeutic areas and treatment analogues for comparison to obesity. A targeted literature review identified clinical and economic outcomes research across the therapeutic area analogues. Associated comorbidities, clinical evidence, indirect costs (ie, absenteeism and productivity loss), and direct medical costs were evaluated to determine the relative value of treating obesity.
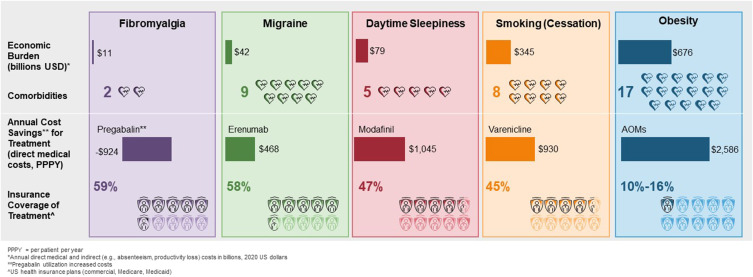
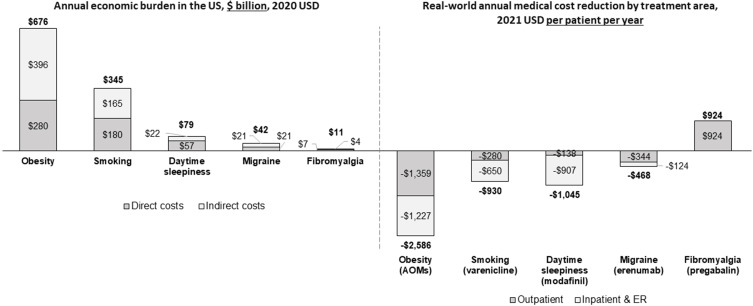
Four therapeutic areas/treatment analogues were selected for comparison to obesity: smoking cessation (varenicline), daytime sleepiness (modafinil), migraines (erenumab), and fibromyalgia (pregabalin). Obesity was associated with 17 comorbidities, more than migraine (9), smoking (8), daytime sleepiness (5), and fibromyalgia (2). Economic burden was greatest for obesity, followed by smoking, with yearly indirect and direct medical costs totaling $676 and $345 billion, respectively. AOMs resulted in cost savings of $2586 in direct medical costs per patient per year (PPPY), greater than that for varenicline at $930 PPPY, modafinil at $1045 PPPY, and erenumab at $468 PPPY; pregabalin utilization increased costs by $924 PPPY. AOMs were covered by 10-16% of United States health insurance plans, compared to 45-59% for the four comparators.
Compared to four therapeutic analogues, obesity represented the highest economic burden and was associated with more comorbidities. AOMs provide greater cost savings compared to selected analogues. However, AOMs have limited formulary coverage. Improved coverage of AOMs may increase access to these treatments and may help address the clinical and economic burden associated with obesity and its comorbidities.
通过比较肥胖症治疗与选定治疗领域的涵盖药物的临床和经济效益,证明有必要改善抗肥胖药物(AOMs)的医疗保险覆盖范围。
通过灰色文献检索,我们确定并优先选择治疗领域和治疗类似物以与肥胖症进行比较。有针对性的文献综述确定了治疗领域类似物的临床和经济结果研究。评估相关合并症、临床证据、间接成本(即旷工和生产力损失)和直接医疗成本,以确定治疗肥胖症的相对价值。
选择了四个治疗领域/治疗类似物与肥胖症进行比较:戒烟(伐尼克兰)、日间嗜睡(莫达非尼)、偏头痛(erenumab)和纤维肌痛(普瑞巴林)。肥胖症与17种合并症相关,多于偏头痛(9种)、吸烟(8种)、日间嗜睡(5种)和纤维肌痛(2种)。肥胖症的经济负担最大,其次是吸烟,每年的间接和直接医疗成本分别总计6760亿美元和3450亿美元。AOMs导致每位患者每年直接医疗成本节省2586美元,高于伐尼克兰的每位患者每年930美元、莫达非尼的每位患者每年1045美元和erenumab的每位患者每年468美元;普瑞巴林的使用使成本增加了每位患者每年924美元。美国医疗保险计划中10%-16%涵盖AOMs,而四种对照药物的这一比例为45%-59%。
与四种治疗类似物相比,肥胖症的经济负担最高,且合并症更多。与选定的类似物相比,AOMs能节省更多成本。然而,AOMs的医保覆盖范围有限。改善AOMs的覆盖范围可能会增加这些治疗的可及性,并有助于解决与肥胖症及其合并症相关的临床和经济负担。