Khara Tanya, Myatt Mark, Sadler Kate, Bahwere Paluku, Berkley James A, Black Robert E, Boyd Erin, Garenne Michel, Isanaka Sheila, Lelijveld Natasha, McDonald Christine, Mertens Andrew, Mwangome Martha, O'Brien Kieran, Stobaugh Heather, Taneja Sunita, West Keith P, Briend André
Emergency Nutrition Network, ENN, 2nd Floor, Marlborough House, 69 High St, Kidlington, OX5 2DN, UK.
Brixton Health, Llwyngwril, Gwynedd, Wales, UK.
Public Health Nutr. 2023 Apr;26(4):803-819. doi: 10.1017/S136898002300023X. Epub 2023 Feb 3.
To understand which anthropometric diagnostic criteria best discriminate higher from lower risk of death in children and explore programme implications.
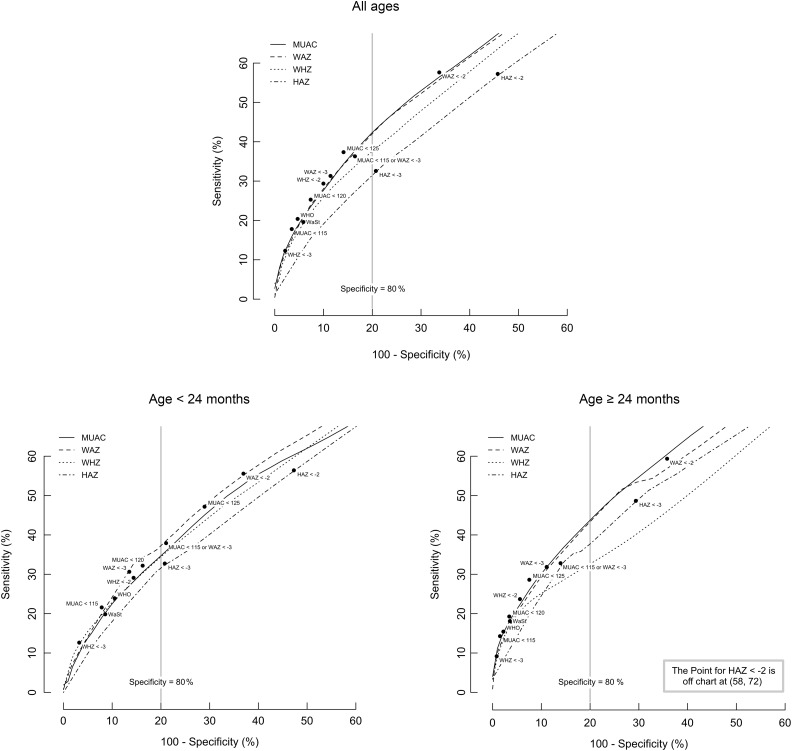
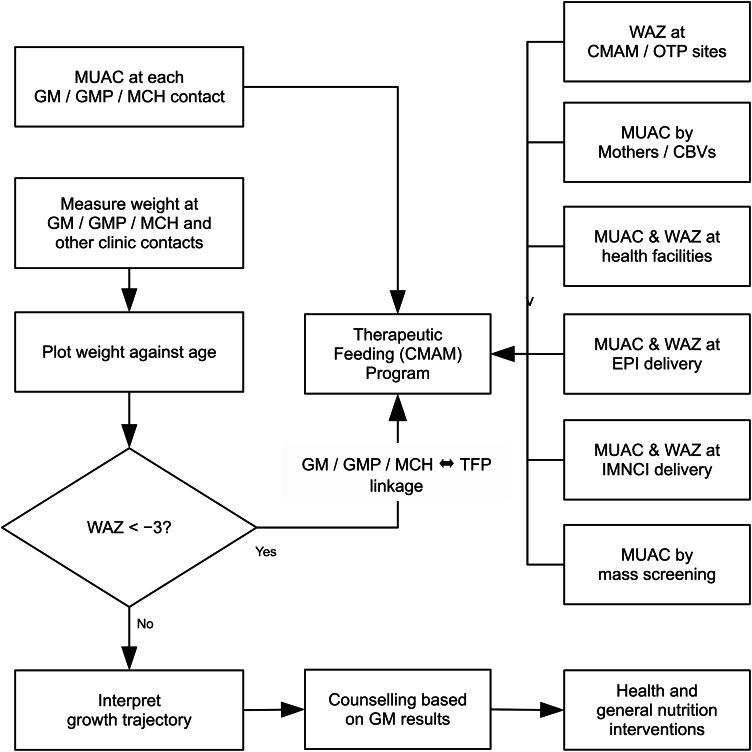
A multiple cohort individual data meta-analysis of mortality risk (within 6 months of measurement) by anthropometric case definitions. Sensitivity, specificity, informedness and inclusivity in predicting mortality, face validity and compatibility with current standards and practice were assessed and operational consequences were modelled.
Community-based cohort studies in twelve low-income countries between 1977 and 2013 in settings where treatment of wasting was not widespread.
Children aged 6 to 59 months.
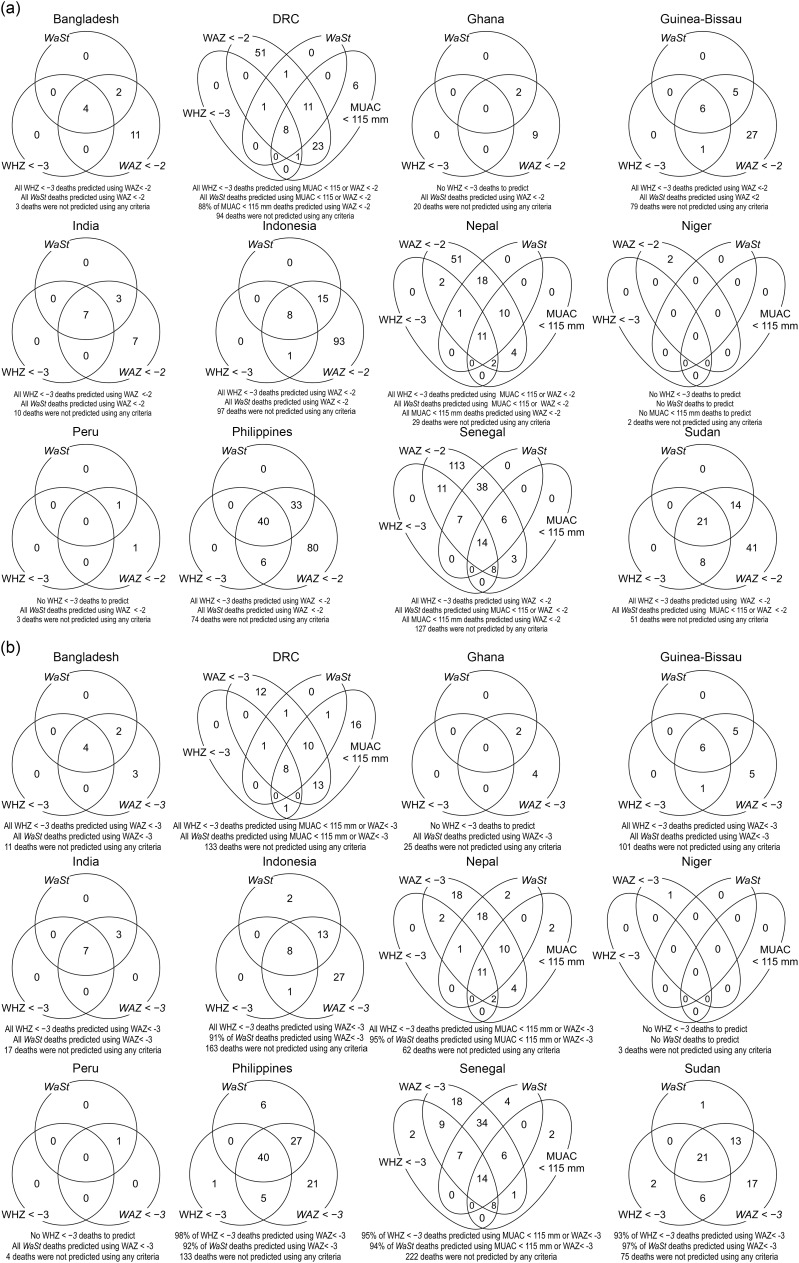
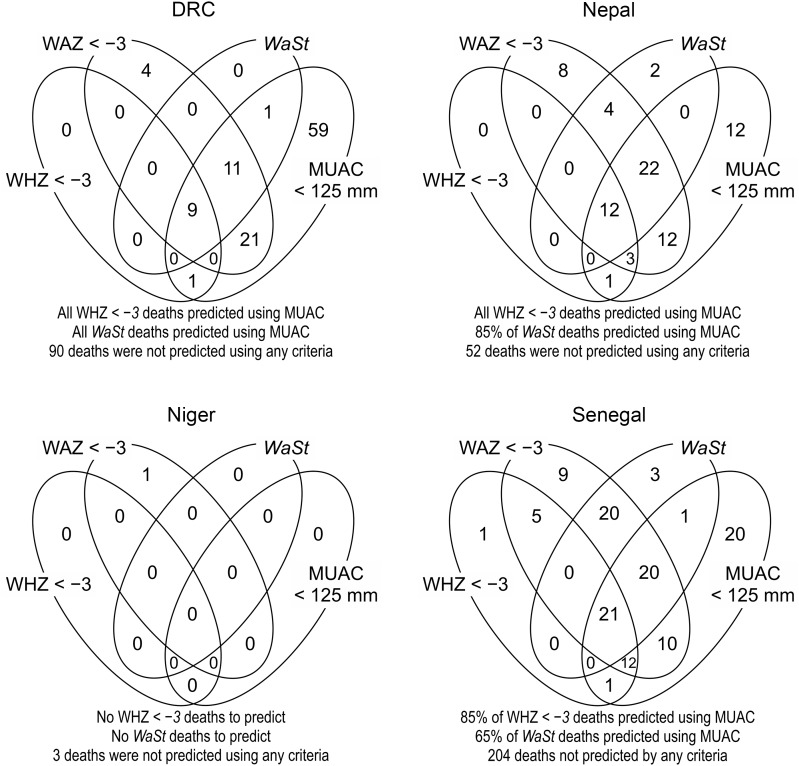
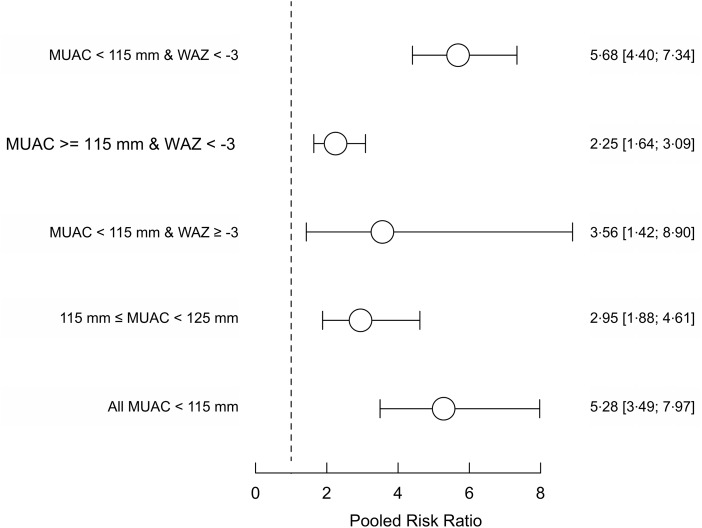
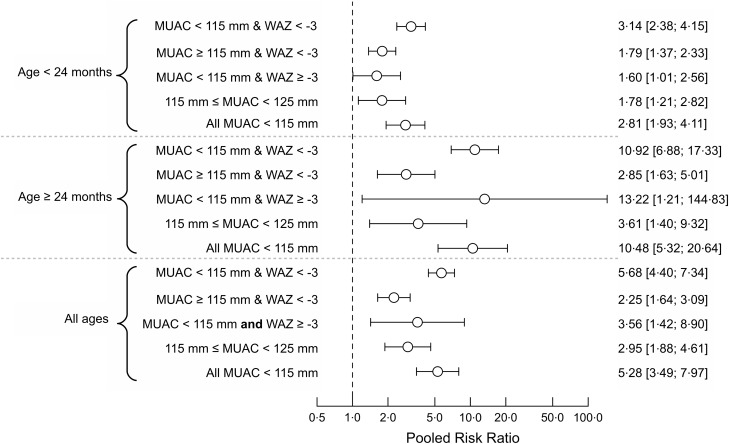
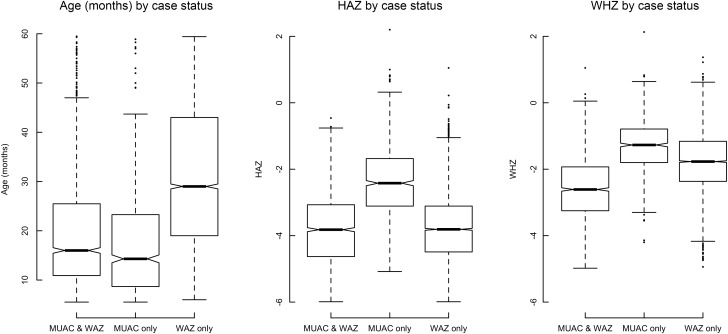
Of the twelve anthropometric case definitions examined, four (weight-for-age -score (WAZ) <-2), (mid-upper arm circumference (MUAC) <125 mm), (MUAC < 115 mm or WAZ < -3) and (WAZ < -3) had the highest informedness in predicting mortality. A combined case definition (MUAC < 115 mm or WAZ < -3) was better at predicting deaths associated with weight-for-height -score <-3 and concurrent wasting and stunting (WaSt) than the single WAZ < -3 case definition. After the assessment of all criteria, the combined case definition performed best. The simulated workload for programmes admitting based on MUAC < 115 mm or WAZ < -3, when adjusted with a proxy for required intensity and/or duration of treatment, was 1·87 times larger than programmes admitting on MUAC < 115 mm alone.
A combined case definition detects nearly all deaths associated with severe anthropometric deficits suggesting that therapeutic feeding programmes may achieve higher impact (prevent mortality and improve coverage) by using it. There remain operational questions to examine further before wide-scale adoption can be recommended.
了解哪些人体测量诊断标准能最有效地区分儿童死亡风险的高低,并探讨对项目的影响。
一项多队列个体数据荟萃分析,根据人体测量病例定义分析(测量后6个月内的)死亡风险。评估了预测死亡率的敏感性、特异性、信息量和包容性、表面效度以及与现行标准和实践的兼容性,并对操作后果进行了建模。
1977年至2013年期间在12个低收入国家开展的基于社区的队列研究,这些地区消瘦治疗并不普遍。
6至59个月大的儿童。
在所研究的12种人体测量病例定义中,四种(年龄别体重评分(WAZ)<-2)、(上臂中部周长(MUAC)<125毫米)、(MUAC<115毫米或WAZ<-3)和(WAZ<-3)在预测死亡率方面具有最高的信息量。与单一的WAZ<-3病例定义相比,综合病例定义(MUAC<115毫米或WAZ<-3)在预测与身高别体重评分<-3以及同时存在的消瘦和发育迟缓(WaSt)相关的死亡方面表现更好。在评估所有标准后,综合病例定义表现最佳。根据MUAC<115毫米或WAZ<-3收治儿童的项目,在用治疗所需强度和/或持续时间的替代指标进行调整后,模拟工作量比仅根据MUAC<115毫米收治儿童的项目大1.87倍。
综合病例定义能检测出几乎所有与严重人体测量缺陷相关的死亡,这表明治疗性喂养项目使用该定义可能会产生更高的影响(预防死亡并提高覆盖率)。在建议广泛采用之前,仍有一些操作问题需要进一步研究。