Odei Obeng-Amoako Gloria Adobea, Myatt Mark, Conkle Joel, Muwaga Brenda Kaijuka, Aryeetey Richmond, Okwi Andrew Livex, Okullo Isaac, Mupere Ezekiel, Wamani Henry, Briend André, Karamagi Charles Amnon Sunday, Kalyango Joan Nakayaga
Clinical Epidemiology Unit, School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda.
Brixton Health, Powys, UK.
Matern Child Nutr. 2020 Oct;16(4):e13000. doi: 10.1111/mcn.13000. Epub 2020 Mar 25.
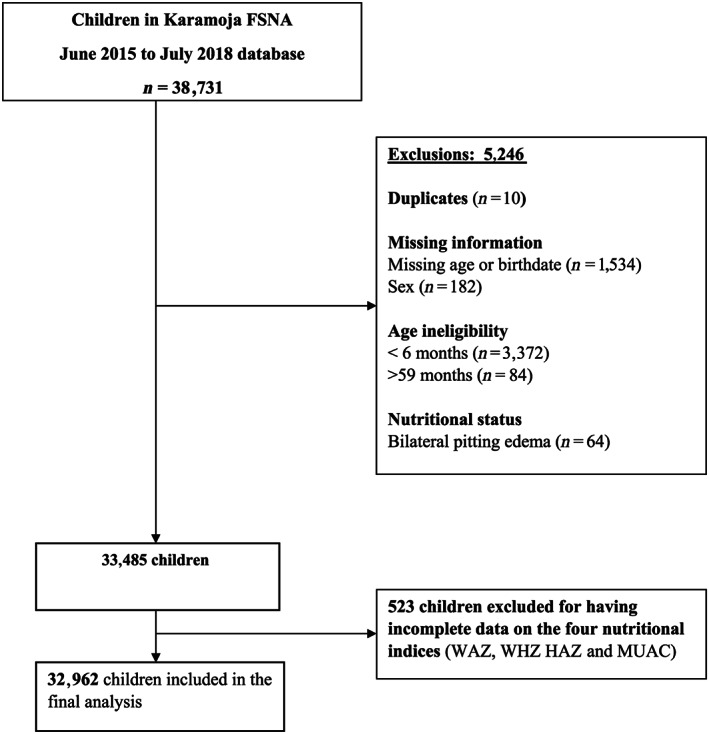
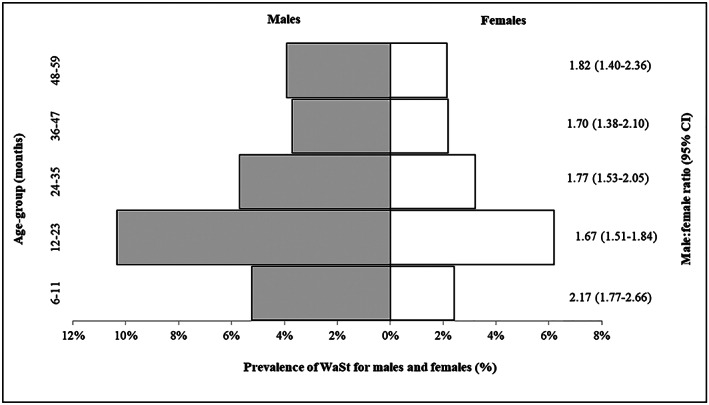
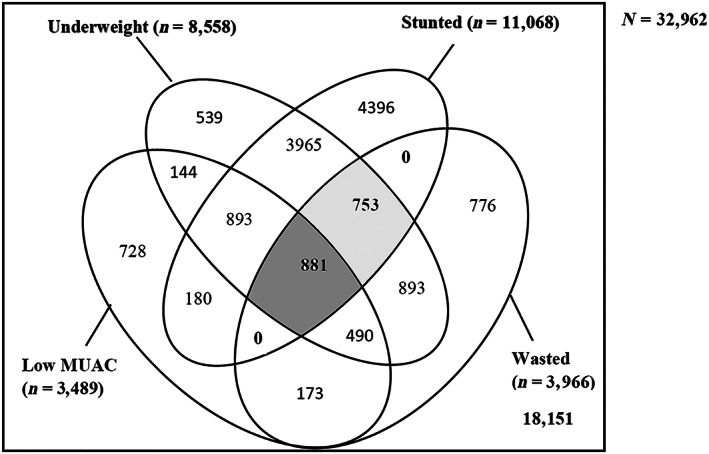
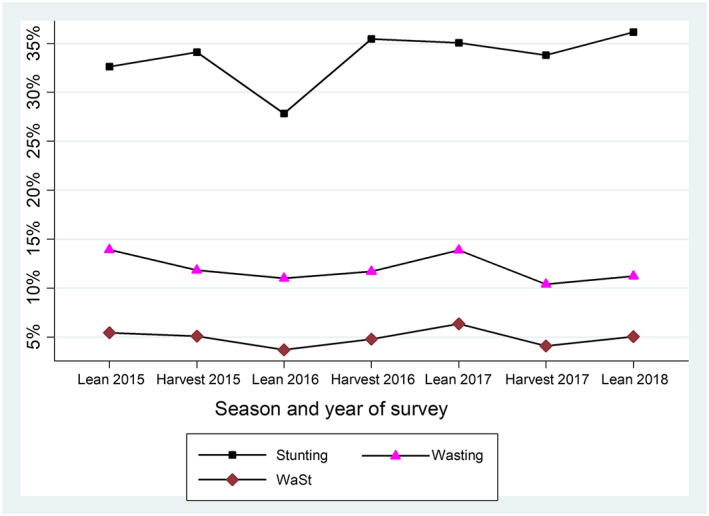
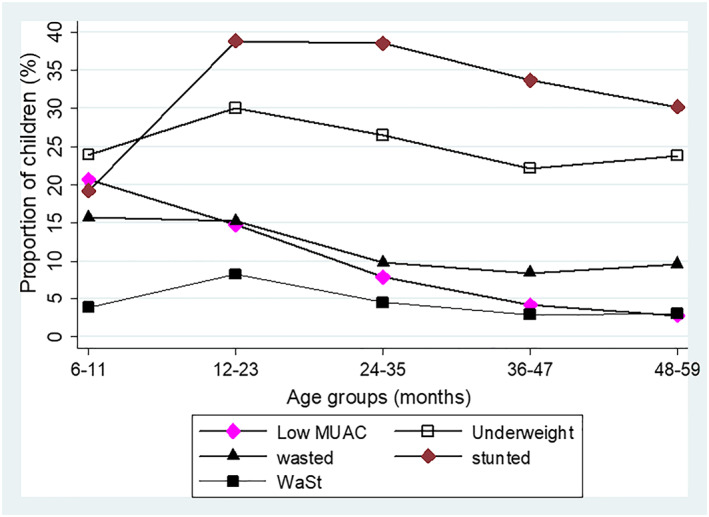
We assessed prevalence of concurrently wasted and stunted (WaSt) and explored the overlaps between wasted, stunted, underweight and low mid-upper arm circumference (MUAC) among children aged 6-59 months in Karamoja, Uganda. We also determined optimal weight-for-age (WAZ) and MUAC thresholds for detecting WaSt. We conducted secondary data analysis with 2015-2018 Food Security and Nutrition Assessment (FSNA) cross-sectional survey datasets from Karamoja. Wasting, stunting and underweight were defined as <-2.0 z-scores using WHO growth standards. Low MUAC was defined as <12.5 cm. We defined WaSt as concurrent wasting and stunting. Prevalence of WaSt was 4.96% (95% CI [4.64, 5.29]). WaSt was more prevalent in lean than harvest season (5.21% vs. 4.53%; p = .018). About half (53.92%) of WaSt children had low MUAC, and all were underweight. Younger children aged <36 months had more WaSt, particularly males. Males with WaSt had higher median MUAC than females (12.50 vs. 12.10 cm; p < .001). A WAZ <-2.60 threshold detected WaSt with excellent sensitivity (99.02%) and high specificity (90.71%). MUAC threshold <13.20 cm had good sensitivity (81.58%) and moderate specificity (76.15%) to detect WaSt. WaSt prevalence of 5% is a public health concern, given its high mortality risk. All children with WaSt were underweight and half had low MUAC. WAZ and MUAC could be useful tools for detecting WaSt. Prevalence monitoring and prospective studies on WAZ and MUAC cut-offs for WaSt detection are recommended. Future consideration to integrate WAZ into therapeutic feeding programmes is recommended to detect and treat WaSt children.
我们评估了乌干达卡拉莫贾6至59个月儿童中同时存在消瘦和发育迟缓(WaSt)的患病率,并探讨了消瘦、发育迟缓、体重不足与低上臂中部周长(MUAC)之间的重叠情况。我们还确定了用于检测WaSt的最佳年龄别体重(WAZ)和MUAC阈值。我们对2015 - 2018年卡拉莫贾粮食安全与营养评估(FSNA)横断面调查数据集进行了二次数据分析。消瘦、发育迟缓和体重不足按照世界卫生组织生长标准定义为z评分<-2.0。低MUAC定义为<12.5厘米。我们将WaSt定义为同时存在消瘦和发育迟缓。WaSt的患病率为4.96%(95%置信区间[4.64, 5.29])。WaSt在青黄不接季节比收获季节更普遍(5.21%对4.53%;p = 0.018)。约一半(53.92%)的WaSt儿童MUAC较低,且全部体重不足。年龄<36个月的幼儿中WaSt更多,尤其是男性。患有WaSt的男性中位MUAC高于女性(12.50对12.10厘米;p<0.001)。WAZ<-2.60的阈值检测WaSt具有极佳的敏感性(99.02%)和较高的特异性(90.71%)。MUAC阈值<13.20厘米检测WaSt具有良好的敏感性(81.58%)和中等特异性(76.15%)。鉴于其高死亡风险,5%的WaSt患病率是一个公共卫生问题。所有患有WaSt的儿童均体重不足,且一半MUAC较低。WAZ和MUAC可能是检测WaSt的有用工具。建议对WaSt检测的WAZ和MUAC临界值进行患病率监测和前瞻性研究。建议未来考虑将WAZ纳入治疗性喂养计划以检测和治疗患有WaSt的儿童。