Department of Epidemiology and Biostatistics, University of California San Francisco, San Francisco, USA.
Department of Epidemiology and Biostatistics, University of California San Francisco, San Francisco, USA; Department of Oncology, Geneva University Hospital, Geneva, Switzerland.
ESMO Open. 2023 Feb;8(1):100779. doi: 10.1016/j.esmoop.2022.100779. Epub 2023 Feb 1.
The statistical plan of a phase II trial should balance minimizing the premature termination of potentially beneficial therapies (i.e. false negatives) and the further, costly testing of ineffective drugs (i.e. false positives). We sought to examine the methodology, reporting, and bias in the interpretation of outcomes of phase II oncology trials in recent years.
In a retrospective cross-sectional analysis, we reviewed all full-length articles published on PubMed from 1 January 2021 to 20 June 2022. We searched for data regarding the sample size calculation (number, α value, power, and expected effect size), the primary and secondary outcomes and results, and the authors' conclusion of the study.
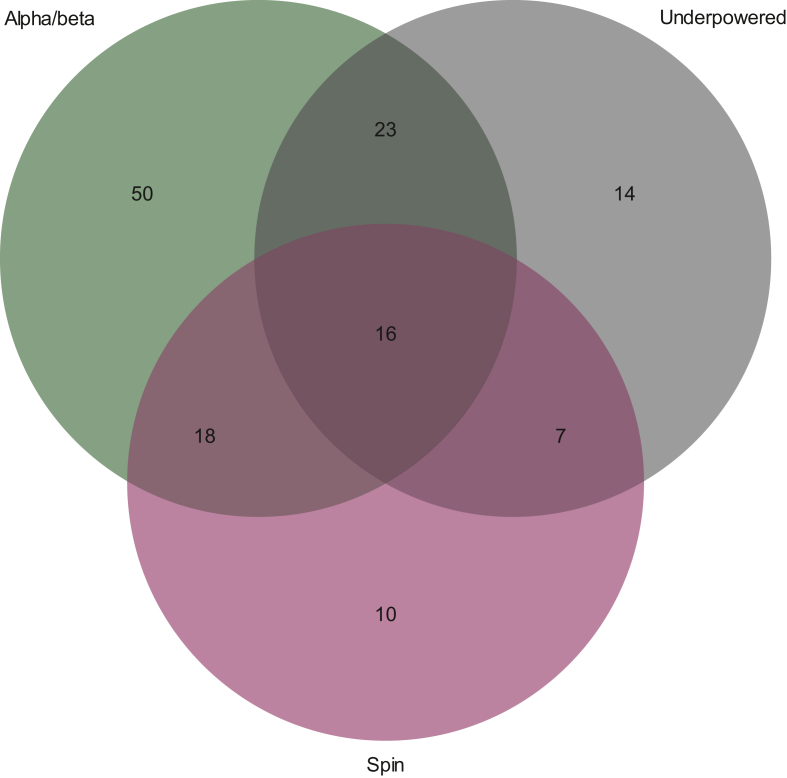
About 5.4% of studies (n = 10) used a statistical power that was inferior to 80%, and 16.7% (n = 34) did not indicate the level of power for the sample size calculation. Approximately 16.7% (n = 31) of studies used a one-sided α level of ≤0.025; 17.7% (n = 33) of studies used a predefined threshold (no comparator effect size or difference between groups) to determine the sample size for efficacy. The percentage of studies with a positive authors' conclusion but not meeting the primary endpoint, or the endpoint was equivocal, was 27.4% (n = 51).
Many randomized phase II studies in oncology failed to report essential data for determining sample size calculations, many did not actually use a comparator to determine efficacy even though the studies were randomized, and many had positive conclusions even though the results were indeterminate or the primary endpoint was not met.
二期临床试验的统计计划应平衡最小化潜在有效治疗方法的过早终止(即假阴性)和进一步昂贵的无效药物测试(即假阳性)。我们试图检查近年来肿瘤学二期临床试验结果的方法学、报告和解释偏倚。
在回顾性横断面分析中,我们复习了 2021 年 1 月 1 日至 2022 年 6 月 20 日期间在 PubMed 上发表的所有全文文章。我们检索了关于样本量计算(数量、α 值、功效和预期效应大小)、主要和次要结局和结果以及作者对研究结论的数据。
约 5.4%(n=10)的研究使用的统计功效低于 80%,16.7%(n=34)未表明样本量计算的功效水平。约 16.7%(n=31)的研究使用单侧α值≤0.025;17.7%(n=33)的研究使用预设阈值(无对照效果大小或组间差异)来确定疗效的样本量。作者得出阳性结论但未达到主要终点或终点不确定的研究比例为 27.4%(n=51)。
许多肿瘤学的随机二期研究未能报告确定样本量计算所需的基本数据,许多研究即使是随机的也没有实际使用对照来确定疗效,许多研究有阳性结论,尽管结果不确定或主要终点未达到。