Infectious Diseases Unit, Department of Internal Medicine, University Hospital of Ferrol, Sergas. Ferrol, 15405, A Coruña, Spain.
, C/ San Amaro 10-12, 6º Derecha, Ferrol, 15403, A Coruña, Spain.
BMC Infect Dis. 2023 Feb 3;23(1):69. doi: 10.1186/s12879-023-08018-0.
Studies have reported increased incidence of BSI over the past decades and indicate that it is necessary to investigate the causes. The aim of this study was to determine the factors affecting trends in the incidence of bacteraemias and associated mortality.
We conducted a retrospective cohort study assessing prospectively collected data of all clinically significant bacteraemias between 1991 and 2020 in a 450-bed hospital. We determined the evolution of bacteraemia-associated incidence, adjusted 30-day mortality and performed multivariable logistic regression to compare the evolution of variables associated with mortality between 5-year periods.
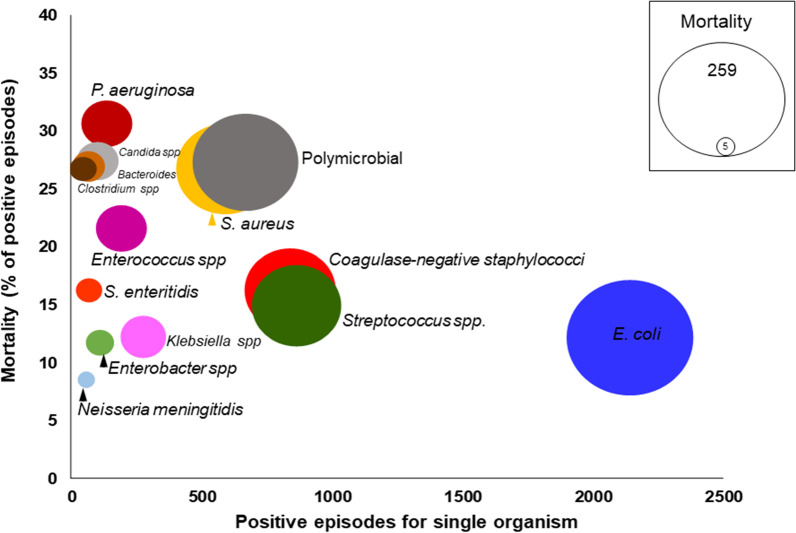
6777 episodes were included, 59.7% males, age 66.5 ± 18.2, 39.4% ≥ 75 years. The incidence total increased: 43.8/100,000/year in 1991-1995 to 205 in 2016-2020; community-acquired bacteraemia (24.9 to 139) and hospital-acquired (0.36/1000 inpatients-days to 1.09). Bacteraemia with source in vascular catheter, urinary and biliary tract increased. The 30-day mortality rate of patients was 1179/6777 (17.4%) in the whole series and population-adjusted mortality incidence increased from 11.4/100,000 in 1991-1996 to 28.4 in 2016-2020 (RR 2.49, 95% CI 2.01-3.08). Mortality was higher in men (18.2% vs 16.3%) and those over 74 years (22.2% vs 14.3%). Appropriate empirical antimicrobial treatment improved (66.5% to 73.1%), 30-day mortality of patients decreased from 26.1 to 13.9%. When comparing the evolution of the factors associated with mortality between 1991 and 1996 vs 2016-2020, the frequency of some variables associated with higher mortality increased: male sex (OR 1.38, 95% CI 1.10-1,74), age (OR 1.02, 1.01-10.3), immunosuppressive treatment (OR 3.1, 2.09-4.6), polymicrobial bacteraemia (OR 1.76, 1.12-2.79), and others decreased: severe sepsis/septic shock (OR 0.70, 0.52-0.93), spontaneous bacterial peritonitis in cirrhosis (OR 0.06, 0.02-0.23), endocarditis (OR 0.54, 0.35-0.83); on the other hand, the frequency of factors associated with lower mortality increased: urinary (OR 1.67, 95% CI 1.23-2.27) and bile tract source (OR 1.59, 1.04-2.43), and adequate empirical treatment (OR 1.42, 95% CI 1.10-1.83).
The incidence of bacteraemia increased due to more elderly, co-morbid patients undergoing procedures and more device related bacteraemia. The percentage of mortality decreased because adequate empirical treatment improved, decreased spontaneous bacterial peritonitis in cirrhosis and endocarditis, and increased bacteraemia of urinary and biliary tract source.
研究报告称,过去几十年来菌血症的发病率有所增加,并表明有必要调查其原因。本研究旨在确定影响菌血症发病率和相关死亡率趋势的因素。
我们进行了一项回顾性队列研究,评估了 1991 年至 2020 年间在一家拥有 450 张床位的医院中所有临床显著菌血症的前瞻性收集数据。我们确定了菌血症相关发病率的演变,调整了 30 天死亡率,并进行了多变量逻辑回归分析,以比较 5 年期间与死亡率相关的变量的演变。
共纳入 6777 例患者,其中男性占 59.7%,年龄 66.5±18.2 岁,39.4%≥75 岁。总发病率增加:1991-1995 年为 43.8/100,000/年,2016-2020 年为 205;社区获得性菌血症(24.9 至 139)和医院获得性菌血症(0.36/1000 住院患者日至 1.09)。血管导管、尿路和胆道来源的菌血症增加。整个系列和人群调整后的患者 30 天死亡率为 1179/6777(17.4%),从 1991-1996 年的 11.4/100,000 增加到 2016-2020 年的 28.4(RR 2.49,95%CI 2.01-3.08)。男性(18.2%比 16.3%)和 74 岁以上的患者死亡率更高(22.2%比 14.3%)。适当的经验性抗菌治疗有所改善(66.5%至 73.1%),患者 30 天死亡率从 26.1%降至 13.9%。当比较 1991 年至 1996 年与 2016 年至 2020 年期间与死亡率相关的因素的演变时,与更高死亡率相关的一些变量的频率增加:男性(OR 1.38,95%CI 1.10-1.74)、年龄(OR 1.02,1.01-10.3)、免疫抑制治疗(OR 3.1,2.09-4.6)、多微生物菌血症(OR 1.76,1.12-2.79),而其他变量则降低:严重脓毒症/败血症(OR 0.70,0.52-0.93)、肝硬化自发性细菌性腹膜炎(OR 0.06,0.02-0.23)、心内膜炎(OR 0.54,0.35-0.83);另一方面,与死亡率较低相关的因素的频率增加:尿路(OR 1.67,95%CI 1.23-2.27)和胆道来源(OR 1.59,1.04-2.43),以及适当的经验性治疗(OR 1.42,95%CI 1.10-1.83)。
由于更多的老年、合并症患者接受了手术,以及更多的与器械相关的菌血症,菌血症的发病率增加。由于适当的经验性治疗有所改善,肝硬化和心内膜炎自发性细菌性腹膜炎减少,以及尿路和胆道来源的菌血症增加,死亡率的百分比下降。