Department of Pediatrics, Emory University, Atlanta, Ga; Division of Pulmonary Medicine, Children's Healthcare of Atlanta, Atlanta, Ga.
Department of Pediatrics, Emory University, Atlanta, Ga; Division of Critical Care Medicine, Children's Healthcare of Atlanta, Atlanta, Ga.
J Allergy Clin Immunol Pract. 2023 May;11(5):1485-1493.e8. doi: 10.1016/j.jaip.2023.01.037. Epub 2023 Feb 3.
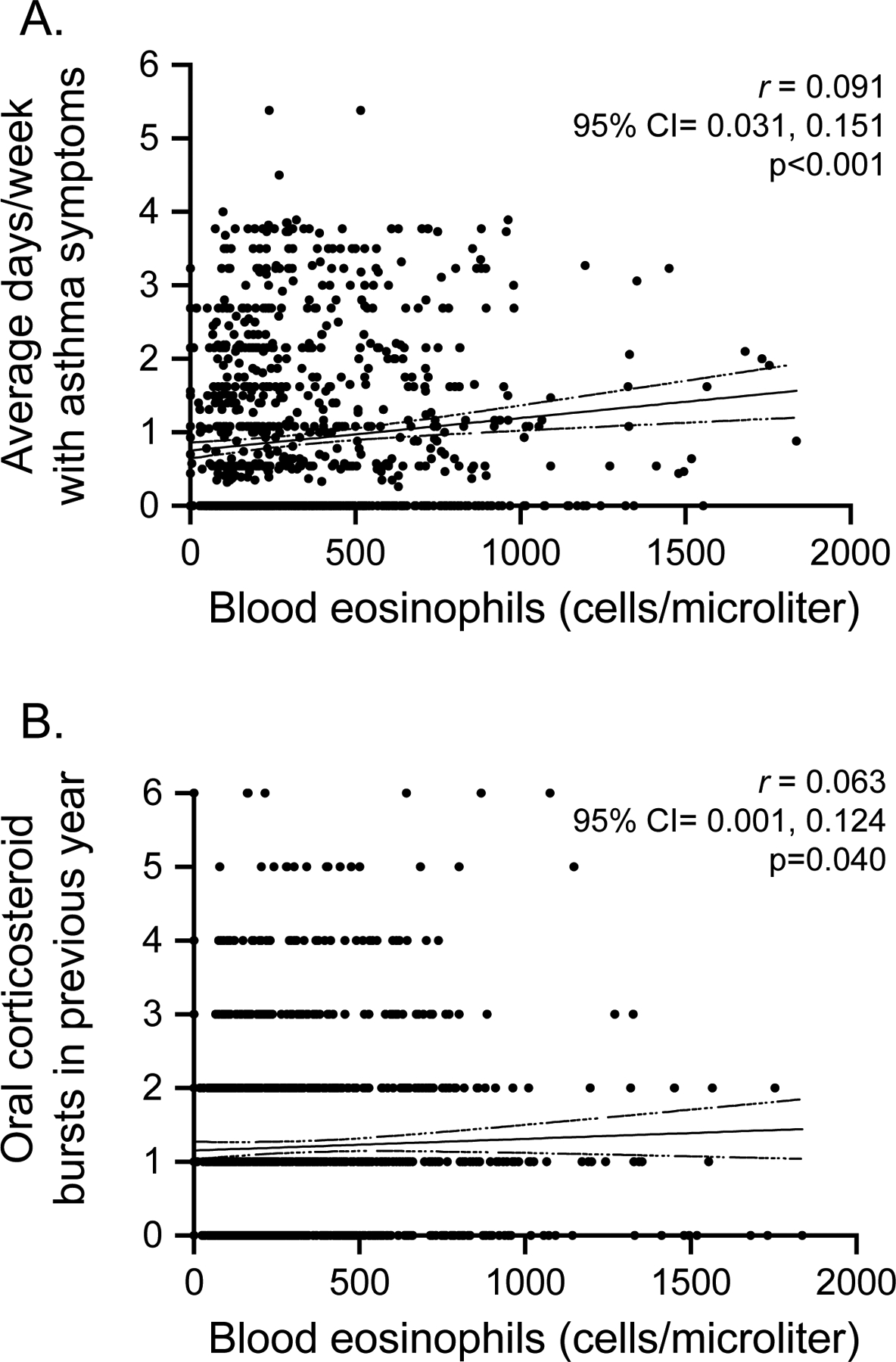
Although clinical features of type 2 inflammation have been associated with poorer longitudinal outcomes in preschool children with recurrent wheezing, it remains difficult to predict which children are at highest risk for poor outcomes during a routine clinical encounter.
We tested the hypothesis that prespecified cut points of blood eosinophil counts would predict exacerbation and treatment response outcomes in preschool children with recurrent wheezing and that prediction could be improved with the addition of a second biomarker.
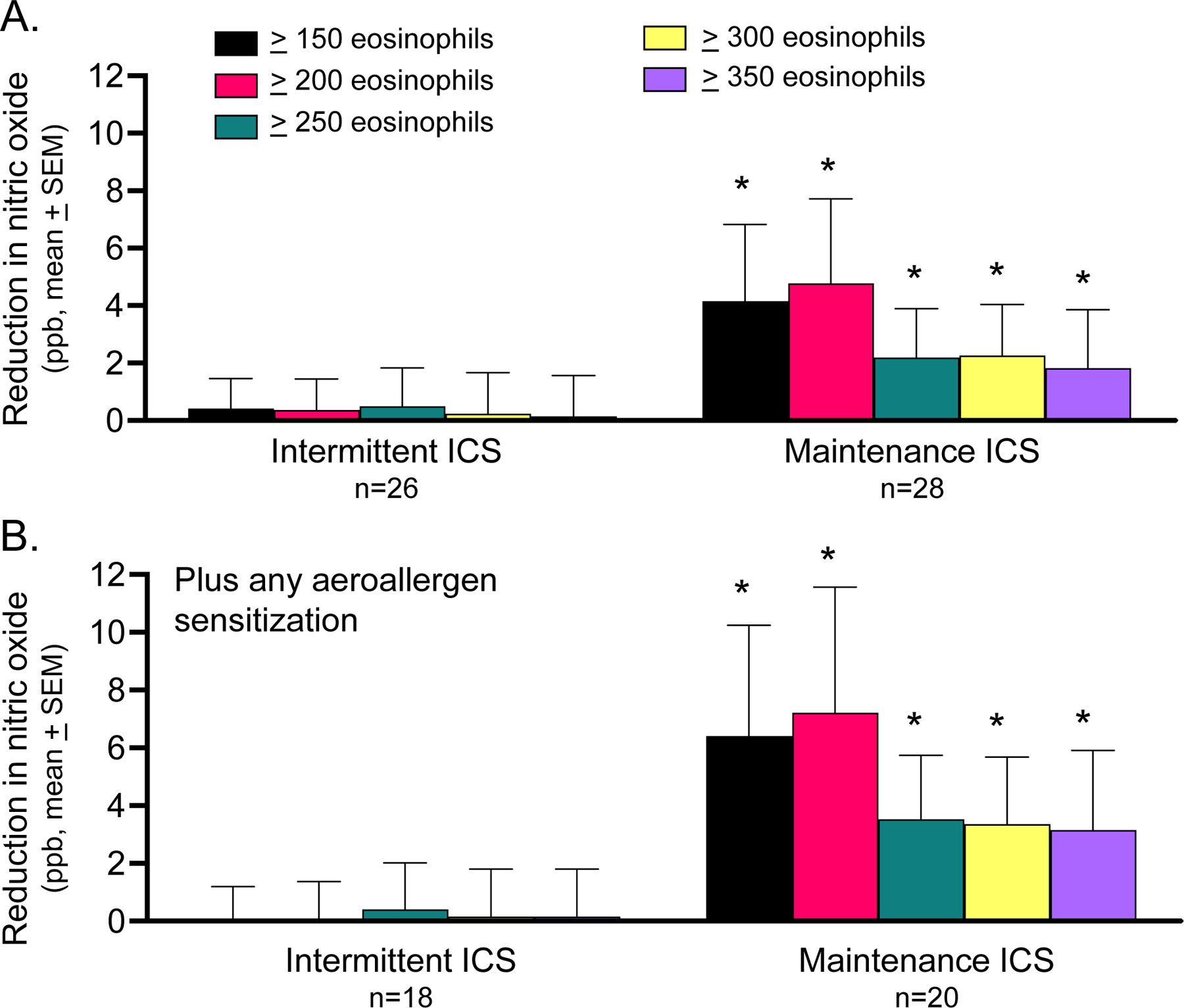
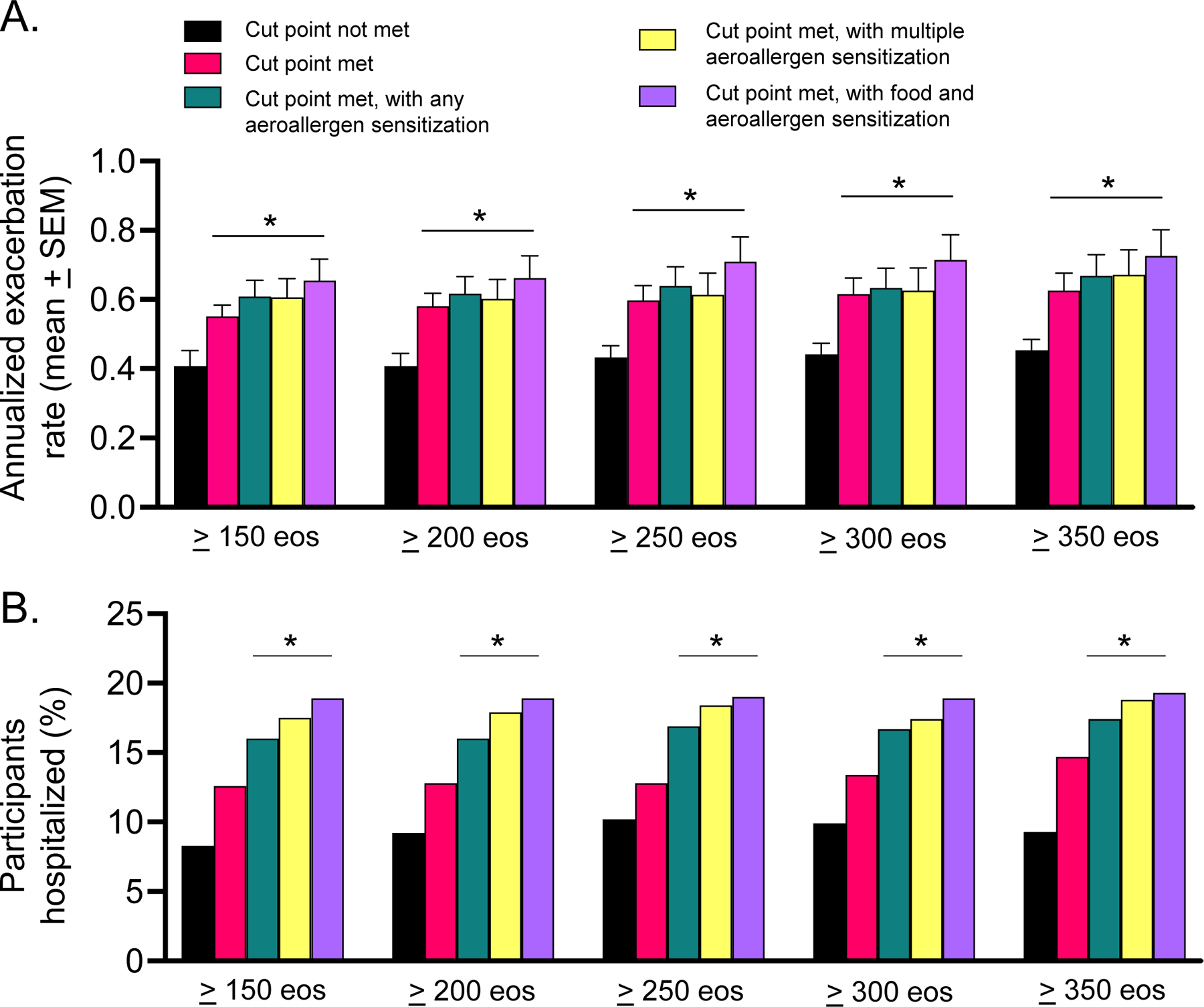
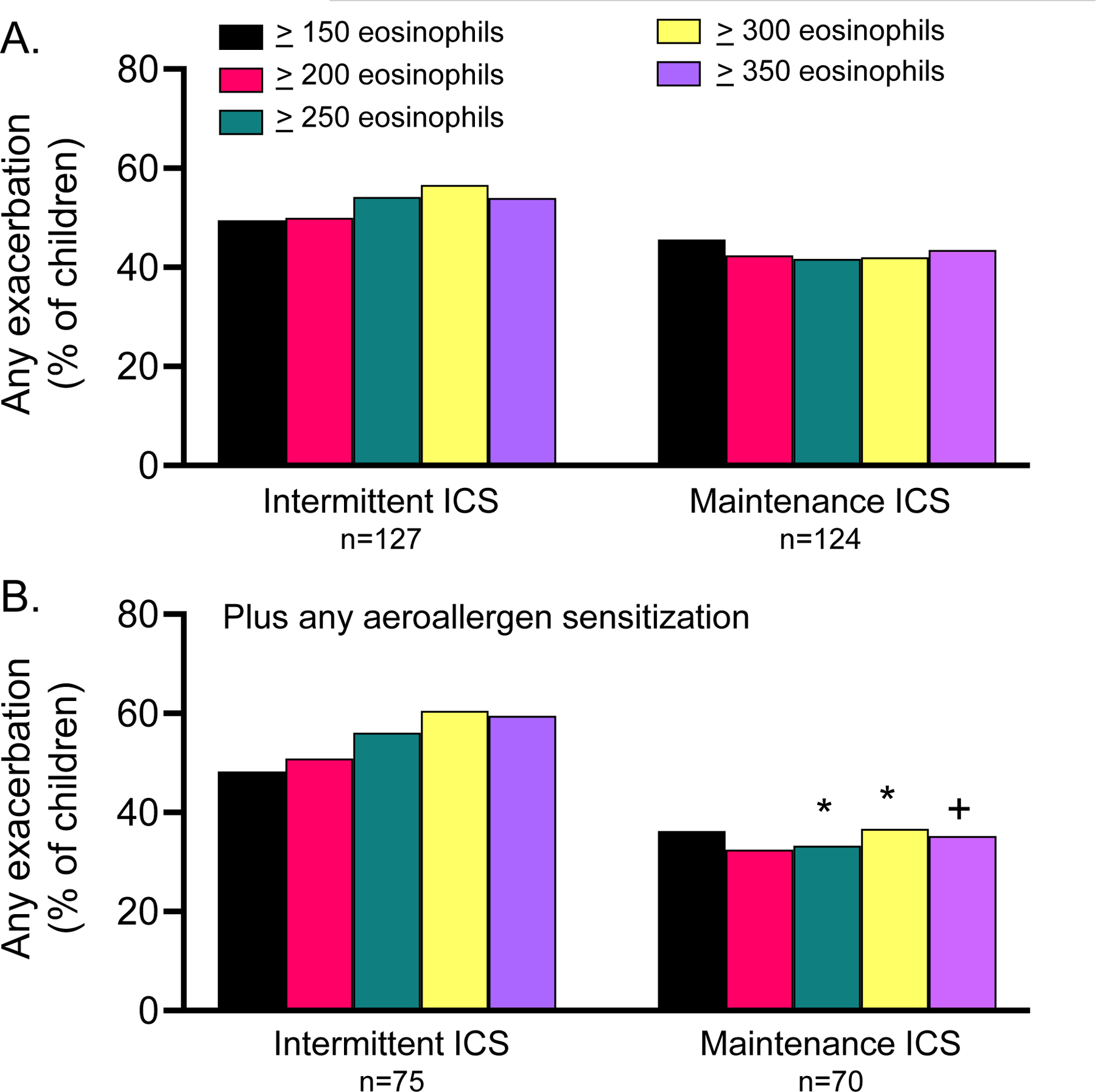
Data from 3 clinical trials of 1,074 preschool children aged 12 to 71 months with recurrent wheezing were merged. The primary outcome was the occurrence of any exacerbation during follow-up. Secondary outcomes included the annualized rate of wheezing exacerbations and the occurrence of any exacerbation requiring hospitalization. Exploratory analyses focused on exacerbation outcomes, offline exhaled nitric oxide concentrations, and caregiver-reported asthma control scores after inhaled corticosteroid treatment initiation.
Each blood eosinophil cut point was associated with increased odds of exacerbation, higher exacerbation rates, and greater hospitalization occurrence in preschool children with recurrent wheezing. However, outcome detection was improved in children with more elevated blood eosinophil counts. Addition of a second biomarker of type 2 inflammation improved outcome detection and was further associated with an improved response to initiation of daily inhaled corticosteroids in exploratory analyses. However, the specificity of blood eosinophils was poor.
Although validation studies are warranted, blood eosinophil cut points may be useful for clinical assessment and future studies of exacerbation and treatment response in preschool children with recurrent wheezing.
尽管 2 型炎症的临床特征与学龄前反复喘息儿童的纵向结局较差相关,但在常规临床就诊中,仍难以预测哪些儿童发生不良结局的风险最高。
我们检验了如下假设,即预设的血嗜酸性粒细胞计数切点可预测学龄前反复喘息儿童的喘息加重和治疗反应结局,并且通过添加第二个生物标志物可改善预测效果。
合并了 3 项学龄前反复喘息儿童(年龄 12~71 个月)临床试验的数据。主要结局是随访期间发生任何喘息加重。次要结局包括喘息加重的年化发生率和需要住院的任何喘息加重的发生情况。探索性分析主要集中在喘息加重结局、离线呼出气一氧化氮浓度和吸入皮质激素治疗开始后照顾者报告的哮喘控制评分。
在学龄前反复喘息儿童中,每个血嗜酸性粒细胞切点均与喘息加重的可能性增加、加重率升高和住院发生率增加相关。然而,在血嗜酸性粒细胞计数更高的儿童中,结局检测得到改善。添加第 2 个 2 型炎症生物标志物可改善结局检测效果,并且在探索性分析中与吸入皮质激素每日治疗起始后的反应改善相关。然而,血嗜酸性粒细胞的特异性较差。
虽然需要验证性研究,但血嗜酸性粒细胞切点可能有助于学龄前反复喘息儿童的临床评估和未来的喘息加重及治疗反应研究。