de Carvalho Daniel Carneiro, Fonseca Francisco Antonio Helfenstein, Izar Maria Cristina de Oliveira, Silveira Ana Luíza Pereira Assunção, Tuleta Izabela Dorota, do Amaral Jônatas Bussador, Neves Lucas Melo, Bachi André Luis Lacerda, França Carolina Nunes
Post Graduation Program in Health Sciences, Santo Amaro University, Sao Paulo, Brazil.
Department of Medicine, Cardiology Division, Federal University of Sao Paulo, Sao Paulo, Brazil.
Front Physiol. 2023 Jan 20;13:1056466. doi: 10.3389/fphys.2022.1056466. eCollection 2022.
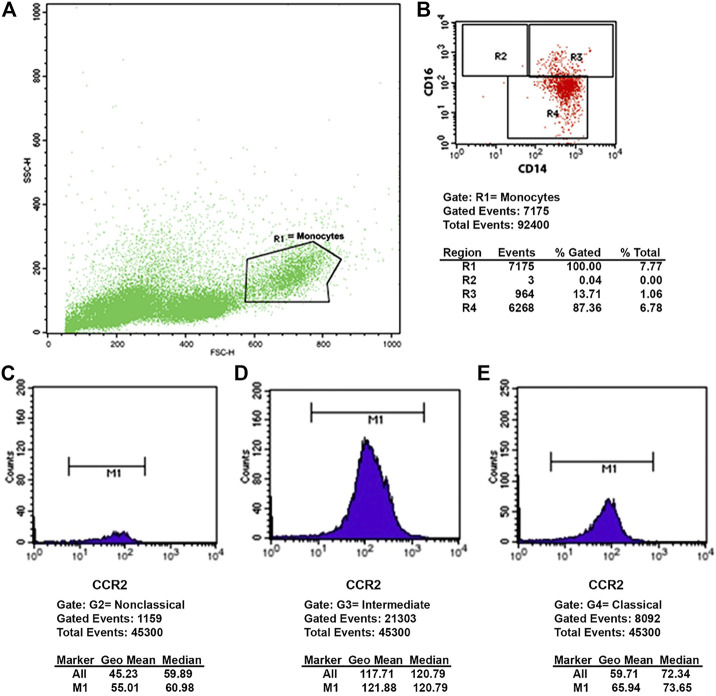
Although it is broadly known that monocyte recruitment is involved in atherosclerosis development and that, in accordance with the microenvironment, these cells can be modulated into three well-known subpopulations: Classical (CD14++CD16-), intermediate (CD14++CD16+), and non-classical (CD14+CD16++), the effects of treatment with different pharmacological strategies (based on lipid-lowering and antiplatelets) after acute myocardial infarction upon the monocytes modulation and the role of the chemokine receptors CCR2, CCR5 and CX3CR1 in this context, are poorly understood. In this study, patients [n = 148, both men (n = 105, 71%) and women (n = 43, 29%)] submitted to treatment with a 2×2 factorial design, in which they received rosuvastatin 20 mg or simvastatin 40 mg plus ezetimibe 10 mg, as well as ticagrelor 90 mg or clopidogrel 75 mg were enrolled. Monocyte subsets were analyzed by flow cytometry at baseline (BL), and after one (1-M) and 6 months (6-M) of treatment. Firstly, our results showed that, regardless of the treatment received, higher percentages of classical monocytes and lower of non-classical monocytes were found at the 6-M time point than BL values, whilst the percentage of intermediate monocytes was higher in all time points assessed than the other subsets. There were reductions in the CCR2 expression by non-classical and intermediate monocytes, without differences for the classical subtype. Concerning the CCR5 expression, there were reductions in the three monocyte subtypes, whereas the CX3CR1 expression increased both in intermediate and classical monocytes, without differences for non-classical monocytes. In relation to the treatment received, a higher percentage of intermediate monocytes at the 6-M time point than the values BL was observed in the group treated with simvastatin + ezetimibe + clopidogrel. No significant differences were found concerning non-classical, intermediate, and classical monocytes, for CCR2, CCR5, and CX3CR1 in the four treatment arms. Taken together, our results demonstrated that even under lipid-lowering and antiplatelet therapy for 6 months, the inflammatory phenotype of monocytes still persisted in the patients enrolled in this study.
虽然人们普遍知道单核细胞募集参与动脉粥样硬化的发展,并且根据微环境,这些细胞可被调节为三个众所周知的亚群:经典型(CD14++CD16-)、中间型(CD14++CD16+)和非经典型(CD14+CD16++),但急性心肌梗死后不同药理策略(基于降脂和抗血小板)治疗对单核细胞调节的影响以及趋化因子受体CCR2、CCR5和CX3CR1在此背景下的作用却知之甚少。在本研究中,纳入了采用2×2析因设计进行治疗的患者[n = 148,男性(n = 105,71%)和女性(n = 43,29%)],他们接受瑞舒伐他汀20 mg或辛伐他汀40 mg加依折麦布10 mg,以及替格瑞洛90 mg或氯吡格雷75 mg治疗。在基线(BL)、治疗1个月(1-M)和6个月(6-M)后通过流式细胞术分析单核细胞亚群。首先,我们的结果表明,无论接受何种治疗,在6-M时间点发现经典单核细胞的百分比高于BL值,而非经典单核细胞的百分比低于BL值,同时在所有评估时间点中间单核细胞的百分比均高于其他亚群。非经典和中间单核细胞的CCR2表达降低,经典亚型无差异。关于CCR5表达,三种单核细胞亚型均降低,而CX3CR1表达在中间和经典单核细胞中均增加,非经典单核细胞无差异。关于所接受的治疗,在辛伐他汀+依折麦布+氯吡格雷治疗组中,观察到6-M时间点中间单核细胞的百分比高于BL值。四个治疗组中CCR2、CCR5和CX3CR1在非经典、中间和经典单核细胞方面未发现显著差异。综上所述,我们的结果表明,即使在进行了6个月的降脂和抗血小板治疗后,本研究纳入患者的单核细胞炎症表型仍然持续存在。