Department of Neurosurgery, Great Ormond Street Hospital for Children, London, UK.
Great Ormond Street Institute of Child Health, University College London, London, UK.
Childs Nerv Syst. 2023 May;39(5):1225-1243. doi: 10.1007/s00381-023-05868-6. Epub 2023 Feb 8.
There is no clear consensus regarding the technique of surgical revascularization for moyamoya disease and syndrome (MMD/MMS) in the pediatric population. Previous meta-analyses have attempted to address this gap in literature but with methodological limitations that affect the reliability of their pooled estimates. This meta-analysis aimed to report an accurate and transparent comparison between studies of indirect (IB), direct (DB), and combined bypasses (CB) in pediatric patients with MMD/MMS.
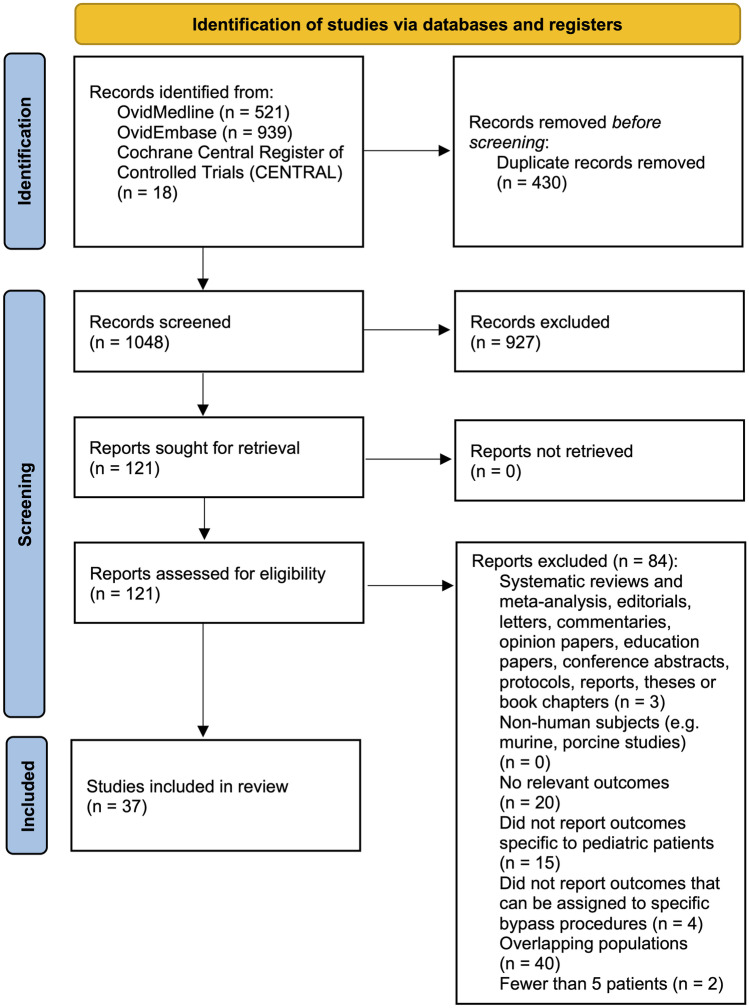
In accordance with PRISMA guidelines, systematic searches of Medline, Embase, and Cochrane Central were undertaken from database inception to 7 October 2022. Perioperative adverse events were the primary outcome measure. Secondary outcomes were rates of long-term revascularization, stroke recurrence, morbidity, and mortality.
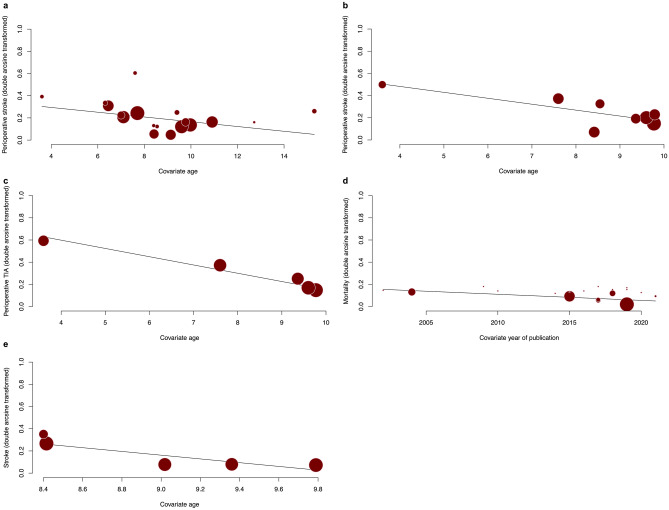
Thirty-seven studies reporting 2460 patients and 4432 hemispheres were included in the meta-analysis. The overall pooled mean age was 8.6 years (95% CI: 7.7; 9.5), and 45.0% were male. Pooled proportions of perioperative adverse events were similar between the DB/CB and IB groups except for wound complication which was higher in the former group (RR = 2.54 (95% CI: 1.82; 3.55)). Proportions of post-surgical Matsushima Grade A/B revascularization favored DB/CB over IB (RR = 1.12 (95% CI 1.02; 1.24)). There was no significant difference in stroke recurrence, morbidity, and mortality. After meta-regression analysis, year of publication and age were significant predictors of outcomes.
IB, DB/CB are relatively effective and safe revascularization options for pediatric MMD/MMS. Low-quality GRADE evidence suggests that DB/CB was associated with better long-term angiographic revascularization outcomes when compared with IB, although this did not translate to long-term stroke and mortality benefits.
对于儿童烟雾病(MMD/MMS),手术再血管化的技术尚无明确共识。之前的荟萃分析试图解决这一文献空白,但存在影响汇总估计可靠性的方法学限制。本荟萃分析旨在报告儿童 MMD/MMS 患者间接(IB)、直接(DB)和联合旁路(CB)之间的准确且透明的比较。
根据 PRISMA 指南,从数据库创建到 2022 年 10 月 7 日,对 Medline、Embase 和 Cochrane Central 进行了系统检索。围手术期不良事件是主要结局指标。次要结局指标是长期再血管化、卒中复发、发病率和死亡率。
共有 37 项研究报告了 2460 名患者和 4432 个半球,纳入了荟萃分析。总体平均年龄为 8.6 岁(95%CI:7.7;9.5),45.0%为男性。DB/CB 和 IB 组的围手术期不良事件发生率相似,但前者的伤口并发症发生率更高(RR=2.54(95%CI:1.82;3.55))。手术后 Matsushima 分级 A/B 再血管化的比例有利于 DB/CB 而不利于 IB(RR=1.12(95%CI 1.02;1.24))。卒中复发、发病率和死亡率无显著差异。元回归分析后,发表年份和年龄是结局的显著预测因素。
IB、DB/CB 是儿童 MMD/MMS 相对有效的安全再血管化选择。低质量的 GRADE 证据表明,与 IB 相比,DB/CB 与更好的长期血管造影再血管化结果相关,尽管这并没有转化为长期卒中获益和死亡率获益。