Department of Urology, University of California, San Francisco, CA, USA.
Department of Epidemiology & Biostatistics, University of California, San Francisco, CA, USA.
Prostate Cancer Prostatic Dis. 2023 Dec;26(4):759-764. doi: 10.1038/s41391-022-00638-y. Epub 2023 Feb 10.
Men with a detectable PSA after radical prostatectomy (RP) are often offered salvage therapy while those with an undetectable PSA are monitored. We aim to better characterize the natural history of men with an initially undetectable PSA who subsequently developed a detectable PSA > 6 months after RP.
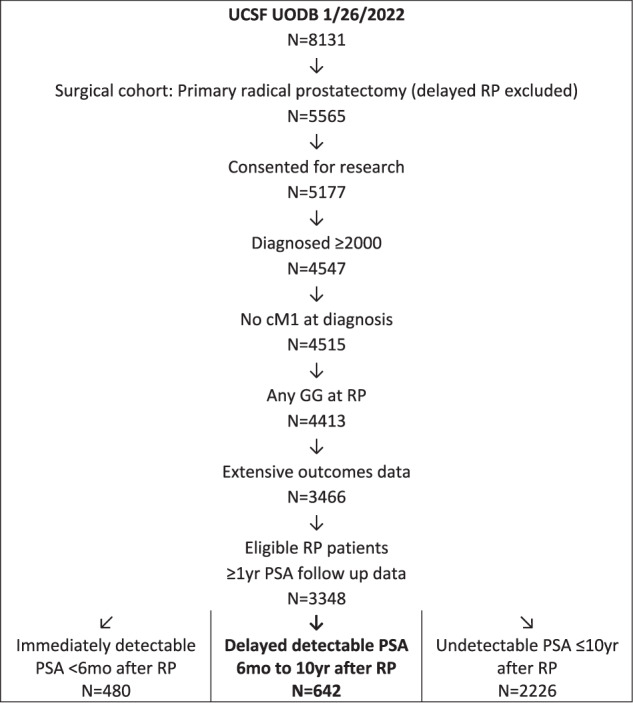
Retrospective analysis of men who underwent RP for clinically localized prostate cancer at the University of California, San Francisco from 2000 to 2022. The primary outcome was biochemical recurrence, defined as 2 consecutive PSA > = 0.03 ng/mL starting 6 months after surgery. Secondary outcomes were salvage treatment, post-salvage treatment, metastasis free survival (MFS), prostate cancer specific mortality (PCSM), and all-cause mortality (ACM). This cohort was compared to a previously described cohort who had an immediately detectable post-operative PSA.
From our cohort of 3348 patients, we identified 2868 men who had an undetectable post-op PSA. Subsequently, 642 men had a delayed detectable PSA at a median of 25 months (IQR 15, 43) with median follow-up of 72 months after RP. PSA at time of failure was <0.10 ng/mL for 65.7% of men. Of those with a delayed detectable PSA, 46% underwent salvage treatment within 10 years after RP at a median PSA of 0.08 ng/mL (IQR 0.05, 0.14). High CAPRA-S score (HR 1.09, CI 1.02-1.17, p = 0.02) and PSA doubling time (PSA-DT) of <6 months (HR 7.58, CI 5.42-10.6, p < 0.01) were associated with receiving salvage treatment. After salvage treatment, 62% of men had recurrent PSA failure within 10 years. Overall, MFS was 92%, PCSM 3%, and ACM 6% at 10 years. For those who received tertiary treatment for recurrent PSA failure, MFS was 54%, PCSM 23% and ACM 23% at 10 years' time.
Men who develop a detectable PSA > 6 months post-operatively may have excellent long-term outcomes, even in the absence of salvage therapy.
根治性前列腺切除术(RP)后 PSA 可检测到的男性通常会接受挽救性治疗,而 PSA 不可检测到的男性则会接受监测。我们旨在更好地描述那些在 RP 后 6 个月后 PSA 可检测到但最初 PSA 不可检测到的男性的自然史。
对 2000 年至 2022 年在加利福尼亚大学旧金山分校接受局限性前列腺癌 RP 的男性进行回顾性分析。主要结局是生化复发,定义为手术后 6 个月开始连续 2 次 PSA≥0.03ng/mL。次要结局是挽救性治疗、挽救性治疗后、无转移生存(MFS)、前列腺癌特异性死亡率(PCSM)和全因死亡率(ACM)。该队列与之前描述的术后即刻可检测到 PSA 的队列进行了比较。
在我们的 3348 例患者队列中,我们确定了 2868 例术后 PSA 不可检测的男性。随后,642 例男性在中位时间 25 个月(IQR 15,43)时出现延迟可检测 PSA,RP 后中位随访时间为 72 个月。失败时 PSA<0.10ng/mL 的男性占 65.7%。在那些延迟可检测 PSA 的患者中,46%的患者在 RP 后 10 年内以中位 PSA 0.08ng/mL(IQR 0.05,0.14)接受挽救性治疗。高 CAPRA-S 评分(HR 1.09,CI 1.02-1.17,p=0.02)和 PSA 倍增时间(PSA-DT)<6 个月(HR 7.58,CI 5.42-10.6,p<0.01)与接受挽救性治疗相关。挽救性治疗后,62%的男性在 10 年内出现 PSA 复发失败。总体而言,MFS 在 10 年内为 92%,PCSM 为 3%,ACM 为 6%。对于那些因 PSA 复发失败而接受三级治疗的患者,MFS 在 10 年内为 54%,PCSM 为 23%,ACM 为 23%。
在 RP 后 6 个月后 PSA 可检测到的男性可能具有出色的长期结局,即使没有挽救性治疗也是如此。