Benda Magdalena A, Ulmer Hanno, Weger Roman, Reimann Patrick, Lang Theresia, Pichler Petra, Winder Thomas, Hartmann Bernd, Strassl Irene, Krauth Maria Theresa, Agis Hermine, Sormann Siegfried, Podar Klaus, Willenbacher Wolfgang, Willenbacher Ella
Internal Medicine II: Oncology, Hematology, Gastroenterology, Infectiology, Academic Teaching Hospital Feldkirch, 6800 Feldkirch, Austria.
Private University of the Principality of Liechtenstein, 9495 Triesen, Principality of Liechtenstein.
Cancers (Basel). 2023 Feb 2;15(3):962. doi: 10.3390/cancers15030962.
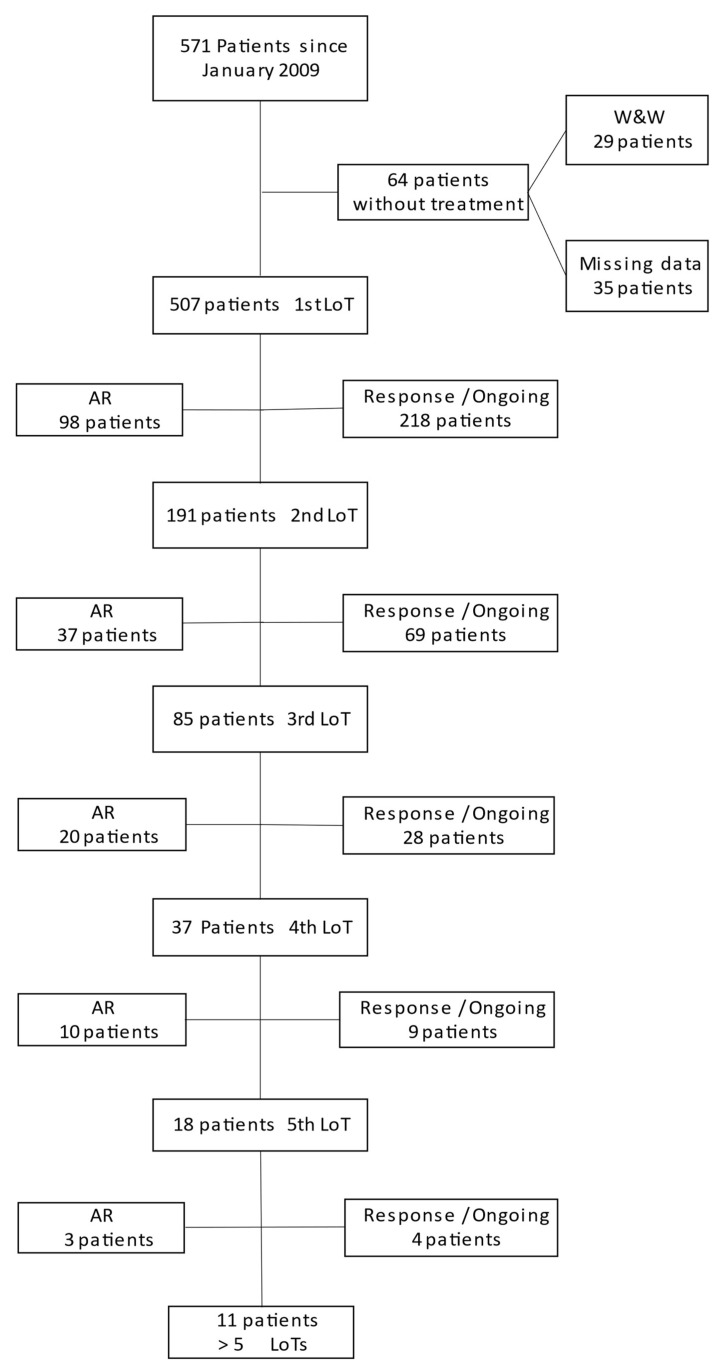
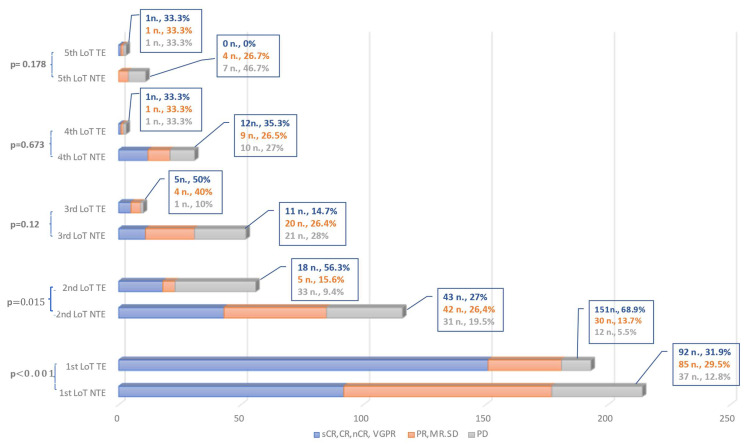
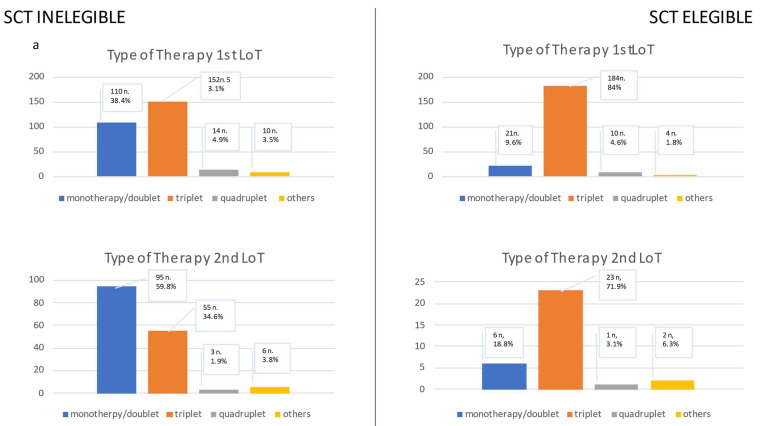
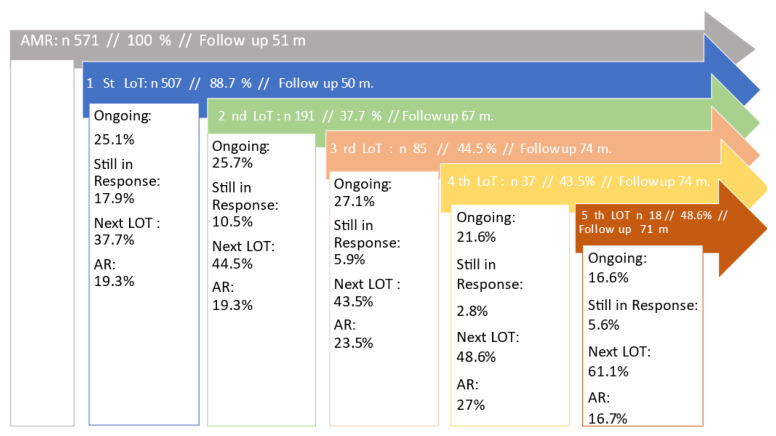
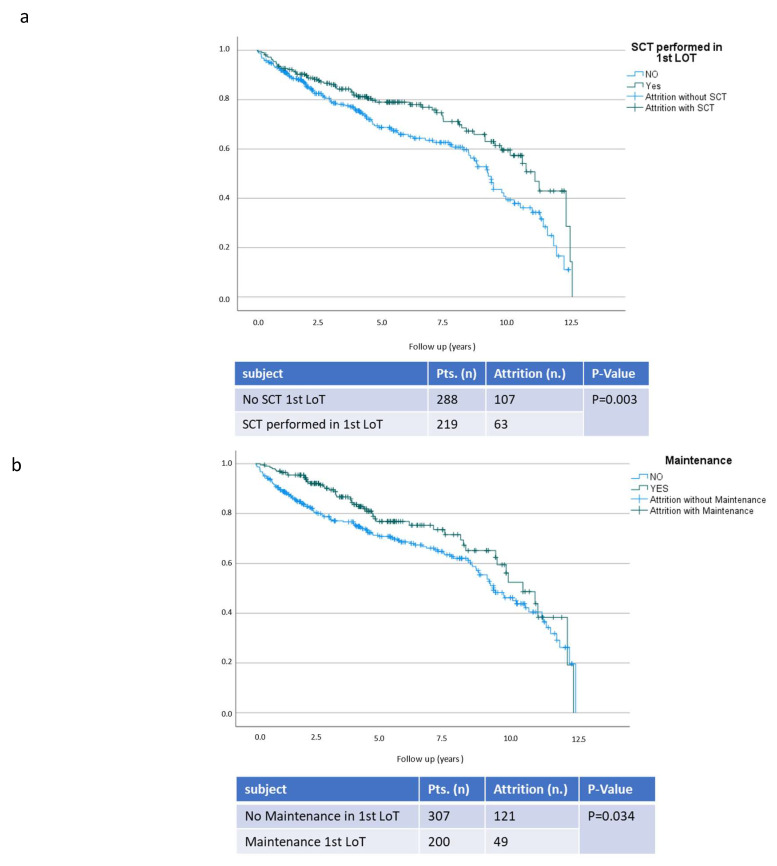
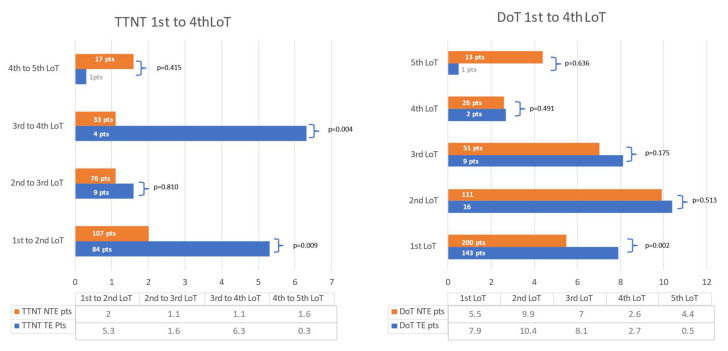
Multiple myeloma (MM) is characterized by serial relapses, necessitating the application of sequential lines of therapy (LoT). Reports on attrition rates (ARs) vary widely. The present study analysed ARs from the Austrian Myeloma Registry. Attrition was defined as being either deceased, progressive without having received another LoT, or lack of follow-up for ≥5 years. A total of 571 patients diagnosed between January 2009 and August 2021 were included (median age: 72 years; median follow-up: 50.8 months). Some 507 patients received at least one LoT. Of the total, 43.6% underwent autologous stem cell transplantation (SCT, transplant eligible = TE)) with primarily VRd (Bortezomib/Lenalidomide/Dexamethasone) given as induction (26.5%), followed by lenalidomide maintenance in 55.7% of cases. Transplant-ineligible (NTE) patients were predominantly treated with Vd (Bortezomib/Dexamethasone, 21.6%), receiving maintenance in 27.1%. A total of 37.5% received a second LoT. ARs across one to five LoTs were 16.7-27%. Frontline induction/ SCT followed by maintenance reduced ARs associated with age and achievement of deep remission in the frontline. Deep remission prolongs follow-up and time-to-next-treatment (TTNT), while high-risk-cyctogenetics negatively affected these outcomes. Our results demonstrate considerably lower ARs for MM patients within the AMR data versus other healthcare systems. Young age and the achievement of significant remissions after optimal frontline therapy resulted in particularly low ARs. These promising results support a key role for the ease of drug access and reimbursement policies in governing long-term MM patient outcomes.
多发性骨髓瘤(MM)的特点是会多次复发,因此需要应用多线治疗方案(LoT)。关于损耗率(AR)的报告差异很大。本研究分析了奥地利骨髓瘤登记处的损耗率。损耗被定义为死亡、病情进展且未接受另一线治疗方案,或随访缺失≥5年。纳入了2009年1月至2021年8月期间诊断的571例患者(中位年龄:72岁;中位随访时间:50.8个月)。约507例患者接受了至少一线治疗方案。其中,43.6%的患者接受了自体干细胞移植(SCT,符合移植条件=TE),诱导治疗主要采用VRd方案(硼替佐米/来那度胺/地塞米松,26.5%),随后55.7%的病例接受来那度胺维持治疗。不符合移植条件(NTE)的患者主要接受Vd方案(硼替佐米/地塞米松,21.6%)治疗,27.1%的患者接受维持治疗。共有37.5%的患者接受了二线治疗方案。一线至五线治疗方案的损耗率为16.7%-27%。一线诱导治疗/SCT后进行维持治疗可降低与年龄相关的损耗率,并提高一线深度缓解率。深度缓解可延长随访时间和下次治疗时间(TTNT),而高危细胞遗传学则对这些结果产生负面影响。我们的结果表明,与其他医疗系统相比,AMR数据中的MM患者损耗率要低得多。年轻以及在最佳一线治疗后实现显著缓解的患者,其损耗率尤其低。这些有前景的结果支持了药物可及性和报销政策在长期MM患者治疗结果管理中的关键作用。