Musculoskeletal Pain and Motor Control Research Group, Faculty of Health Sciences, Universidad Europea de Canarias, 38300 Santa Cruz de Tenerife, Spain.
Musculoskeletal Pain and Motor Control Research Group, Faculty of Sport Sciences, Universidad Europea de Madrid, 28670 Villaviciosa de Odón, Spain.
Int J Environ Res Public Health. 2023 Feb 1;20(3):2617. doi: 10.3390/ijerph20032617.
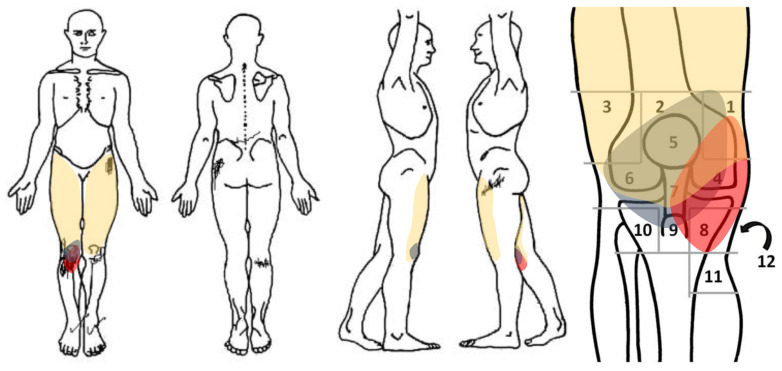
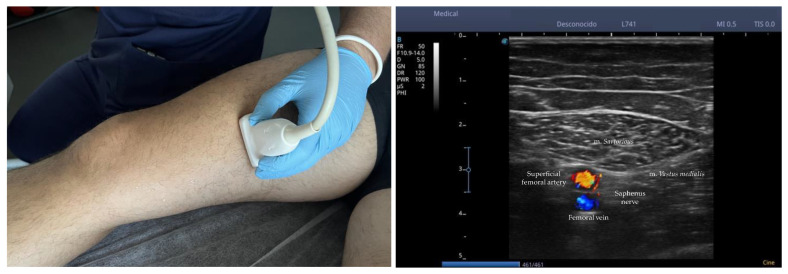
is a neuromuscular transmission disorder characterized by weakness of the cranial and skeletal muscles, however, neuropathies are extremely rare. In this case report we present a case of a 61-year-old man diagnosed who came to our attention due to a 1 week of acute deep pain [NPRS 8/10] in the anterior and medial right knee which occurred during walking [NPRS 8/10] or stair climbing [NPRS 9/10]. A complete medical record and clinical examination based on physical exploration and ultrasound assessment confirmed a infrapatellar saphenous neuralgia. Therapeutic interventions included Percutaneous nerve electrical stimulation combined with pain neuroscience education, neural mobilization of the saphenous nerve and quadriceps resistance exercises. After 4 weeks, pain intensity [NRPS = 1/10], knee functionality [OKS = 41/48] and lower limb functionality [LLFI = 80%] were notably improved, nevertheless, fatigue [RPE = 2/10] was similar than baseline. At 2 months of follow-up, the effect on intensity of pain NRPS [0/10] and functionality OKS [40/48] and LLFI [82%] was maintained, however, no significant clinical changes were detected on perceived fatigue RPE Scale [2/10]. Despite the important methodological limitations of this study, our case report highlights the efficacy of percutaneous electrical nerve stimulation combined with physical agents modalities for pain and functionality of infrapatellar saphenous neuralgia in the context of
这是一种以颅神经和骨骼肌无力为特征的神经肌肉传递障碍,但神经病变极为罕见。在本病例报告中,我们介绍了一位 61 岁男性的病例,他因右膝前内侧深部疼痛[NPRS 8/10]就诊,行走时[NPRS 8/10]或爬楼梯时[NPRS 9/10]出现疼痛。完整的病历和临床检查基于物理探查和超声评估,确认了髌下隐神经痛。治疗干预包括经皮神经电刺激联合疼痛神经科学教育、隐神经和股四头肌阻力运动。4 周后,疼痛强度[NPRS = 1/10]、膝关节功能[NPRS = 41/48]和下肢功能[LLFI = 80%]显著改善,但疲劳[NPRS = 2/10]与基线相似。2 个月随访时,疼痛强度[NPRS = 0/10]、膝关节功能[NPRS = 40/48]和下肢功能[LLFI = 82%]保持不变,但感知疲劳 RPE 量表[2/10]无明显临床变化。尽管本研究存在重要的方法学局限性,但我们的病例报告强调了经皮神经电刺激联合物理因子治疗髌下隐神经痛疼痛和功能的疗效。