Garassino Marina C, Gadgeel Shirish, Novello Silvia, Halmos Balazs, Felip Enriqueta, Speranza Giovanna, Hui Rina, Garon Edward B, Horinouchi Hidehito, Sugawara Shunichi, Rodriguez-Abreu Delvys, Reck Martin, Cristescu Razvan, Aurora-Garg Deepti, Loboda Andrey, Lunceford Jared, Kobie Julie, Ayers Mark, Piperdi Bilal, Pietanza M Catherine, Paz-Ares Luis
Section of Hematology/Oncology, Thoracic Oncology program, University of Chicago, Chicago, Illinois, and IRCCS Istituto Nazionale dei Tumori, Milano.
Division of Hematology/Oncology, Department of Internal Medicine, Henry Ford Cancer Institute/Henry Ford Health System, Detroit, Michigan.
JTO Clin Res Rep. 2022 Nov 8;4(1):100431. doi: 10.1016/j.jtocrr.2022.100431. eCollection 2023 Jan.
We evaluated tissue tumor mutational burden (tTMB) and mutations in and as biomarkers for outcomes with pembrolizumab plus platinum-based chemotherapy (pembrolizumab-combination) for NSCLC among patients in the phase 3 KEYNOTE-189 (ClinicalTrials.gov, NCT02578680; nonsquamous) and KEYNOTE-407 (ClinicalTrials.gov, NCT02775435; squamous) trials.
This retrospective exploratory analysis evaluated prevalence of high tTMB and , and mutations in patients enrolled in KEYNOTE-189 and KEYNOTE-407 and the relationship between these potential biomarkers and clinical outcomes. tTMB and , , and mutation status was assessed using whole-exome sequencing in patients with available tumor and matched normal DNA. The clinical utility of tTMB was assessed using a prespecified cutpoint of 175 mutations/exome.
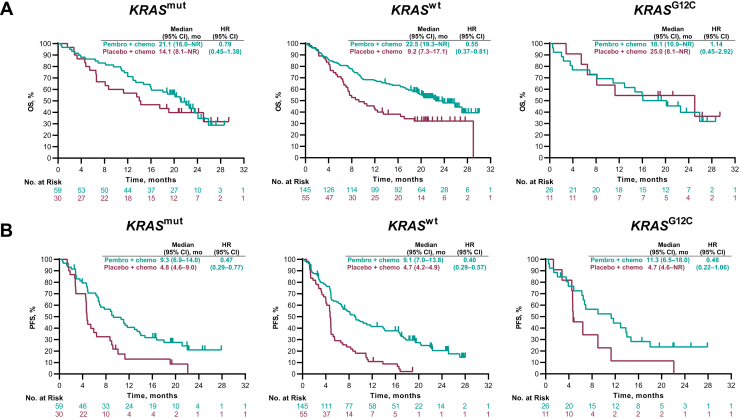
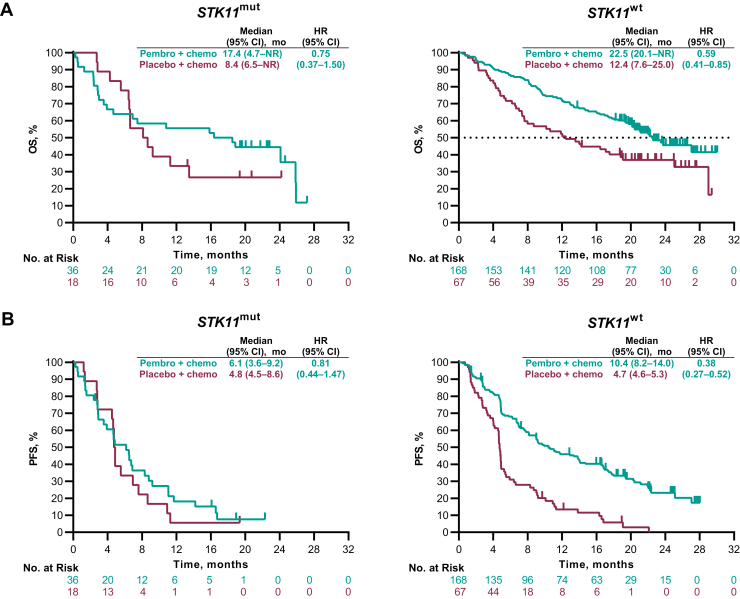
Among patients with evaluable data from whole-exome sequencing for evaluation of tTMB (KEYNOTE-189, = 293; KEYNOTE-407, = 312) and matched normal DNA, no association was found between continuous tTMB score and overall survival (OS) or progression-free survival for pembrolizumab-combination (Wald test, one-sided > 0.05) or placebo-combination (Wald test, two-sided > 0.05) in patients with squamous or nonsquamous histology. Pembrolizumab-combination improved outcomes for patients with tTMB greater than or equal to 175 compared with tTMB less than 175 mutations/exome in KEYNOTE-189 (OS, hazard ratio = 0.64 [95% confidence interval (CI): 0.38‒1.07] and 0.64 [95% CI: 0.42‒0.97], respectively) and KEYNOTE-407 (OS, hazard ratio = 0.74 [95% CI: 0.50‒1.08 and 0.86 [95% CI: 0.57‒1.28], respectively) versus placebo-combination. Treatment outcomes were similar regardless of , or mutation status.
These findings support pembrolizumab-combination as first-line treatment in patients with metastatic NSCLC and do not suggest the utility of tTMB, or mutation status as a biomarker for this regimen.
我们在3期KEYNOTE-189(ClinicalTrials.gov,NCT02578680;非鳞状)和KEYNOTE-407(ClinicalTrials.gov,NCT02775435;鳞状)试验中,评估了组织肿瘤突变负荷(tTMB)以及 和 基因的突变,将其作为帕博利珠单抗联合铂类化疗(帕博利珠单抗联合方案)用于非小细胞肺癌(NSCLC)患者疗效的生物标志物。
这项回顾性探索性分析评估了KEYNOTE-189和KEYNOTE-407试验中入组患者的高tTMB以及 、 和 基因突变的发生率,以及这些潜在生物标志物与临床结局之间的关系。在有可用肿瘤组织及匹配正常DNA的患者中,使用全外显子组测序评估tTMB以及 、 、 基因突变状态。使用预先设定的175个突变/外显子的切点评估tTMB的临床效用。
在有可评估全外显子组测序数据用于评估tTMB(KEYNOTE-189, = 293;KEYNOTE-407, = 312)及匹配正常DNA的患者中,对于鳞状或非鳞状组织学患者,连续tTMB评分与帕博利珠单抗联合方案(Wald检验,单侧 > 0.05)或安慰剂联合方案(Wald检验,双侧 > 0.05)的总生存期(OS)或无进展生存期之间均未发现关联。在KEYNOTE-189中,与tTMB低于175个突变/外显子相比,tTMB大于或等于175的患者接受帕博利珠单抗联合方案时,OS的风险比分别为0.64[95%置信区间(CI):0.38‒1.07]和0.64[95%CI:0.42‒0.97];在KEYNOTE-407中,与安慰剂联合方案相比,OS的风险比分别为0.74[95%CI:0.50‒1.08]和0.86[95%CI:0.57‒1.28]。无论 、 或 基因突变状态如何,治疗结局相似。
这些发现支持帕博利珠单抗联合方案作为转移性NSCLC患者的一线治疗方案,并不表明tTMB、 或 基因突变状态可作为该治疗方案的生物标志物。