Division of Hematology/Oncology, Department of Medicine, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania.
Division of Pulmonary, Allergy and Critical Care Medicine, Department of Medicine, University of Pennsylvania Perelman School of Medicine, Philadelphia, Pennsylvania.
Clin Cancer Res. 2020 May 15;26(10):2354-2361. doi: 10.1158/1078-0432.CCR-19-3663. Epub 2020 Feb 26.
The role of plasma-based tumor mutation burden (pTMB) in predicting response to pembrolizumab-based first-line standard-of-care therapy for metastatic non-small cell lung cancer (mNSCLC) has not been explored.
A 500-gene next-generation sequencing panel was used to assess pTMB. Sixty-six patients with newly diagnosed mNSCLC starting first-line pembrolizumab-based therapy, either alone or in combination with chemotherapy, were enrolled (Clinicaltrial.gov identifier: NCT03047616). Response was assessed using RECIST 1.1. Associations were made for patient characteristics, 6-month durable clinical benefit (DCB), progression-free survival (PFS), and overall survival (OS).
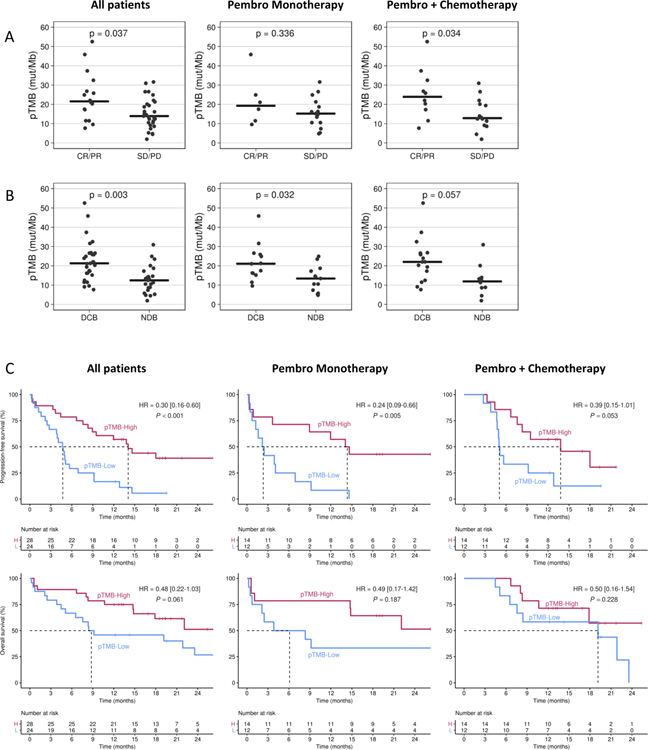
Of 66 patients, 52 (78.8%) were pTMB-evaluable. Median pTMB was 16.8 mutations per megabase (mut/Mb; range, 1.9-52.5) and was significantly higher for patients achieving DCB compared with no durable benefit (21.3 mut/Mb vs. 12.4 mut/Mb, = 0.003). For patients with pTMB ≥ 16 mut/Mb, median PFS was 14.1 versus 4.7 months for patients with pTMB < 16 mut/Mb [HR, 0.30 (0.16-0.60); < 0.001]. Median OS for patients with pTMB ≥ 16 was not reached versus 8.8 months for patients with pTMB < 16 mut/Mb [HR, 0.48 (0.22-1.03); = 0.061]. Mutations in exon 20, , or were more common in patients with no DCB. A combination of pTMB ≥ 16 and absence of negative predictor mutations was associated with PFS [HR, 0.24 (0.11-0.49); < 0.001] and OS [HR, 0.31 (0.13-0.74); = 0.009].
pTMB ≥ 16 mut/Mb is associated with improved PFS after first-line standard-of-care pembrolizumab-based therapy in mNSCLC. and mutations may help identify pTMB-high patients unlikely to respond. These results should be validated in larger prospective studies.
血浆肿瘤突变负荷(pTMB)在预测转移性非小细胞肺癌(mNSCLC)一线标准治疗中接受帕博利珠单抗治疗的反应中的作用尚未得到探索。
使用 500 个基因的下一代测序面板来评估 pTMB。招募了 66 名新诊断为 mNSCLC 且开始接受一线帕博利珠单抗单药或联合化疗治疗的患者(临床试验.gov 标识符:NCT03047616)。使用 RECIST 1.1 评估应答。将患者特征、6 个月持久临床获益(DCB)、无进展生存期(PFS)和总生存期(OS)与 pTMB 相关联。
在 66 名患者中,有 52 名(78.8%)可进行 pTMB 评估。中位 pTMB 为 16.8 个突变/兆碱基(mut/Mb;范围,1.9-52.5),与无持久获益的患者相比,达到 DCB 的患者 pTMB 明显更高(21.3 mut/Mb 比 12.4 mut/Mb, = 0.003)。对于 pTMB≥16 mut/Mb 的患者,中位 PFS 为 14.1 个月,而 pTMB<16 mut/Mb 的患者为 4.7 个月[HR,0.30(0.16-0.60);<0.001]。pTMB≥16 的患者中位 OS 未达到,而 pTMB<16 mut/Mb 的患者为 8.8 个月[HR,0.48(0.22-1.03);=0.061]。无 DCB 的患者中更常见 exon 20、 、 突变。pTMB≥16 且不存在阴性预测突变的组合与 PFS 相关[HR,0.24(0.11-0.49);<0.001]和 OS[HR,0.31(0.13-0.74);=0.009]。
pTMB≥16 mut/Mb 与一线标准治疗帕博利珠单抗治疗后 mNSCLC 的 PFS 改善相关。 和 突变可能有助于识别不太可能应答的 pTMB 高患者。这些结果应在更大的前瞻性研究中得到验证。