Meyer Cancer Center, Weill Cornell Medicine and New York Presbyterian Hospital, New York, NY.
Memorial Sloan Kettering Cancer Center, New York, NY.
Blood. 2023 May 4;141(18):2194-2205. doi: 10.1182/blood.2022018254.
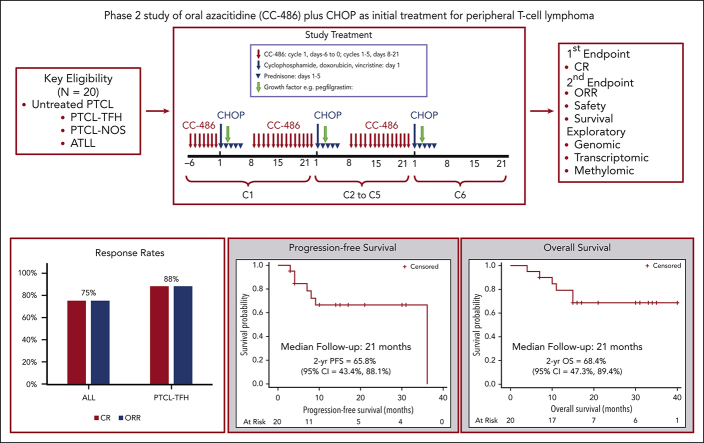
Peripheral T-cell lymphomas (PTCL) with T-follicular helper phenotype (PTCL-TFH) has recurrent mutations affecting epigenetic regulators, which may contribute to aberrant DNA methylation and chemoresistance. This phase 2 study evaluated oral azacitidine (CC-486) plus cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) as initial treatment for PTCL. CC-486 at 300 mg daily was administered for 7 days before C1 of CHOP, and for 14 days before CHOP C2-6. The primary end point was end-of-treatment complete response (CR). Secondary end points included safety and survival. Correlative studies assessed mutations, gene expression, and methylation in tumor samples. Grade 3 to 4 hematologic toxicities were mostly neutropenia (71%), with febrile neutropenia uncommon (14%). Nonhematologic toxicities included fatigue (14%) and gastrointestinal symptoms (5%). In 20 evaluable patients, CR was 75%, including 88.2% for PTCL-TFH (n = 17). The 2-year progression-free survival (PFS) was 65.8% for all and 69.2% for PTCL-TFH, whereas 2-year overall survival (OS) was 68.4% for all and 76.1% for PTCL-TFH. The frequencies of the TET2, RHOA, DNMT3A, and IDH2 mutations were 76.5%, 41.1%, 23.5%, and 23.5%, respectively, with TET2 mutations significantly associated with CR (P = .007), favorable PFS (P = .004) and OS (P = .015), and DNMT3A mutations associated with adverse PFS (P = .016). CC-486 priming contributed to the reprograming of the tumor microenvironment by upregulation of genes related to apoptosis (P < .01) and inflammation (P < .01). DNA methylation did not show significant shift. This safe and active regimen is being further evaluated in the ALLIANCE randomized study A051902 in CD30-negative PTCL. This trial was registered at www.clinicaltrials.gov as #NCT03542266.
外周 T 细胞淋巴瘤(PTCL)伴 T 滤泡辅助表型(PTCL-TFH)存在影响表观遗传调节剂的复发性突变,这可能导致异常的 DNA 甲基化和化疗耐药。这项 2 期研究评估了口服阿扎胞苷(CC-486)联合环磷酰胺、多柔比星、长春新碱和泼尼松(CHOP)作为 PTCL 的初始治疗。CC-486 每天 300mg,在 CHOP 的 C1 前用 7 天,在 CHOP C2-6 前用 14 天。主要终点是治疗结束时的完全缓解(CR)。次要终点包括安全性和生存。相关研究评估了肿瘤样本中的突变、基因表达和甲基化。3 级至 4 级血液学毒性主要为中性粒细胞减少症(71%),发热性中性粒细胞减少症少见(14%)。非血液学毒性包括疲劳(14%)和胃肠道症状(5%)。在 20 例可评估的患者中,CR 为 75%,其中 PTCL-TFH 为 88.2%(n=17)。所有患者的 2 年无进展生存率(PFS)为 65.8%,PTCL-TFH 为 69.2%,所有患者的 2 年总生存率(OS)为 68.4%,PTCL-TFH 为 76.1%。TET2、RHOA、DNMT3A 和 IDH2 突变的频率分别为 76.5%、41.1%、23.5%和 23.5%,TET2 突变与 CR(P=0.007)、有利的 PFS(P=0.004)和 OS(P=0.015)显著相关,DNMT3A 突变与不良的 PFS(P=0.016)相关。CC-486 引发可通过上调与凋亡(P<0.01)和炎症(P<0.01)相关的基因,对肿瘤微环境进行重编程。DNA 甲基化没有明显变化。在 CD30 阴性 PTCL 的 ALLIANCE 随机研究 A051902 中,正在进一步评估这种安全有效的方案。该试验在 www.clinicaltrials.gov 上注册为#NCT03542266。