Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Department of Thoracic Oncology, Peking University Cancer Hospital and Institute, Beijing, China.
Department of Medical Oncology, Cancer Hospital of University of Chinese Academy of Sciences & Zhejiang Cancer Hospital, Hangzhou, China.
J Immunother Cancer. 2023 Feb;11(2). doi: 10.1136/jitc-2022-006055.
Some patients with locally advanced/metastatic non-small cell lung cancer (NSCLC) respond poorly to anti-programmed cell death protein 1 (PD-1)/anti-programmed death-ligand 1 (PD-L1) treatments. Combination with other agents may improve the outcomes. This open-label, multicenter, phase 1b trial investigated the combination of sitravatinib, a spectrum-selective tyrosine kinase inhibitor, plus anti-PD-1 antibody tislelizumab.
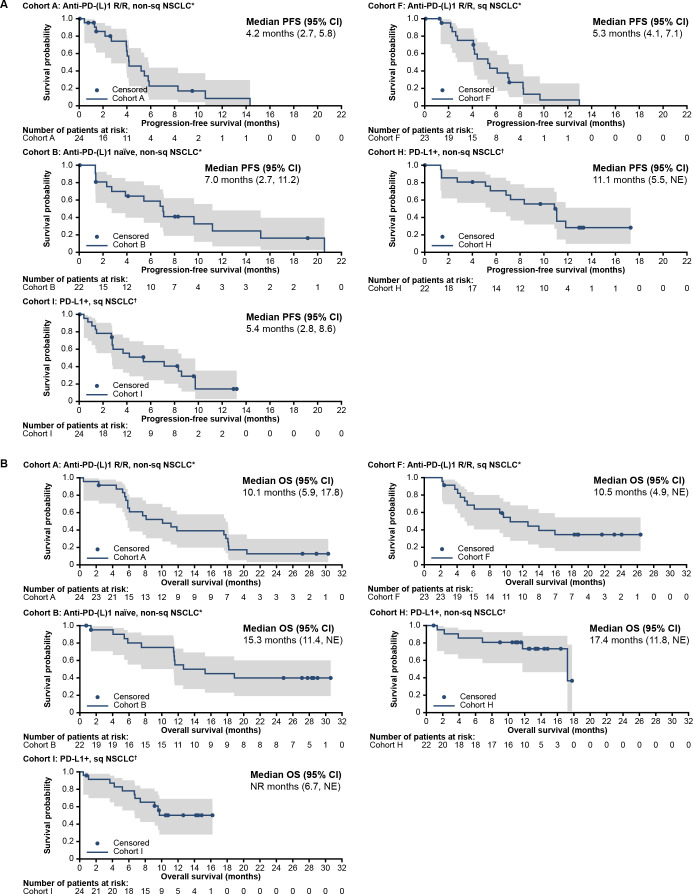
Patients with locally advanced/metastatic NSCLC were enrolled (Cohorts A, B, F, H, and I; N=22-24 per cohort). Cohorts A and F included patients previously treated with systemic therapy, with anti-PD-(L)1-resistant/refractory non-squamous (cohort A) or squamous (cohort F) disease. Cohort B included patients previously treated with systemic therapy, with anti-PD-(L)1-naïve non-squamous disease. Cohorts H and I included patients without prior systemic therapy for metastatic disease, no prior anti-PD-(L)1/immunotherapy, with PD-L1-positive non-squamous (cohort H) or squamous (cohort I) histology. Patients received sitravatinib 120 mg orally one time per day plus tislelizumab 200 mg intravenously every 3 weeks, until study withdrawal, disease progression, unacceptable toxicity, or death. The primary endpoint was safety/tolerability among all treated patients (N=122). Secondary endpoints included investigator-assessed tumor responses and progression-free survival (PFS).
Median follow-up was 10.9 months (range: 0.4-30.6). Treatment-related adverse events (TRAEs) occurred in 98.4% of the patients, with ≥Grade 3 TRAEs in 51.6%. TRAEs led to discontinuation of either drug in 23.0% of the patients. Overall response rate was 8.7% (n/N: 2/23; 95% CI: 1.1% to 28.0%), 18.2% (4/22; 95% CI: 5.2% to 40.3%), 23.8% (5/21; 95% CI: 8.2% to 47.2%), 57.1% (12/21; 95% CI: 34.0% to 78.2%), and 30.4% (7/23; 95% CI: 13.2% to 52.9%) in cohorts A, F, B, H, and I, respectively. Median duration of response was not reached in cohort A and ranged from 6.9 to 17.9 months across other cohorts. Disease control was achieved in 78.3-90.9% of the patients. Median PFS ranged from 4.2 (cohort A) to 11.1 months (cohort H).
In patients with locally advanced/metastatic NSCLC, sitravatinib plus tislelizumab was tolerable for most patients, with no new safety signals and overall safety profiles consistent with known profiles of these agents. Objective responses were observed in all cohorts, including in patients naïve to systemic and anti-PD-(L)1 treatments, or with anti-PD-(L)1 resistant/refractory disease. Results support further investigation in selected NSCLC populations.
NCT03666143.
一些局部晚期/转移性非小细胞肺癌(NSCLC)患者对抗程序性死亡蛋白 1(PD-1)/抗程序性死亡配体 1(PD-L1)治疗反应不佳。联合其他药物可能会改善疗效。这项开放标签、多中心、1b 期试验研究了谱选择性酪氨酸激酶抑制剂司他拉替尼联合抗 PD-1 抗体替雷利珠单抗的联合用药。
招募了局部晚期/转移性 NSCLC 患者(队列 A、B、F、H 和 I;每个队列 22-24 例)。队列 A 和 F 包括先前接受过系统治疗、抗 PD-(L)1 耐药/难治性非鳞状(队列 A)或鳞状(队列 F)疾病的患者。队列 B 包括先前接受过系统治疗、抗 PD-(L)1 初治非鳞状疾病的患者。队列 H 和 I 包括无转移性疾病先前系统治疗、无先前抗 PD-(L)1/免疫治疗、PD-L1 阳性非鳞状(队列 H)或鳞状(队列 I)组织学的患者。患者接受司他拉替尼 120mg 口服,每日一次,联合替雷利珠单抗 200mg 静脉输注,每 3 周一次,直至研究退出、疾病进展、不可接受的毒性或死亡。主要终点是所有治疗患者的安全性/耐受性(N=122)。次要终点包括研究者评估的肿瘤反应和无进展生存期(PFS)。
中位随访时间为 10.9 个月(范围:0.4-30.6)。98.4%的患者发生了与治疗相关的不良事件(TRAEs),≥3 级 TRAEs 发生率为 51.6%。TRAEs 导致 23.0%的患者停止使用这两种药物。总体缓解率为 8.7%(n/N:2/23;95%CI:1.1%至 28.0%),18.2%(4/22;95%CI:5.2%至 40.3%),23.8%(5/21;95%CI:8.2%至 47.2%),57.1%(12/21;95%CI:34.0%至 78.2%)和 30.4%(7/23;95%CI:13.2%至 52.9%)分别在队列 A、F、B、H 和 I 中。队列 A 中未达到缓解持续时间的中位数,其他队列的缓解持续时间从 6.9 个月到 17.9 个月不等。78.3-90.9%的患者达到疾病控制。中位 PFS 范围从队列 A 的 4.2 个月到队列 H 的 11.1 个月。
在局部晚期/转移性 NSCLC 患者中,司他拉替尼联合替雷利珠单抗对大多数患者是可耐受的,没有新的安全性信号,总体安全性与这两种药物已知的安全性一致。所有队列均观察到客观反应,包括对系统治疗和抗 PD-(L)1 治疗均初治的患者,或对 PD-(L)1 耐药/难治性疾病的患者。结果支持在选定的 NSCLC 人群中进一步研究。
NCT03666143。