Department of Upper Abdominal Surgery, Karolinska University Hospital, C1:77, Stockholm, Sweden.
Division of Surgery, Department of Clinical Science, Intervention and Technology (CLINTEC), Karolinska Institutet, Hälsovägen 13, 141 57, Huddinge, Stockholm, Sweden.
Gastric Cancer. 2023 May;26(3):467-477. doi: 10.1007/s10120-023-01371-8. Epub 2023 Feb 19.
Laparoscopic gastrectomy is increasingly used for the treatment of locally advanced gastric cancer but concerns remain whether similar results can be obtained compared to open gastrectomy, especially in Western populations. This study compared the short-term postoperative, oncological and survival outcomes following laparoscopic versus open gastrectomy based on data from the Swedish National Register for Esophageal and Gastric Cancer.
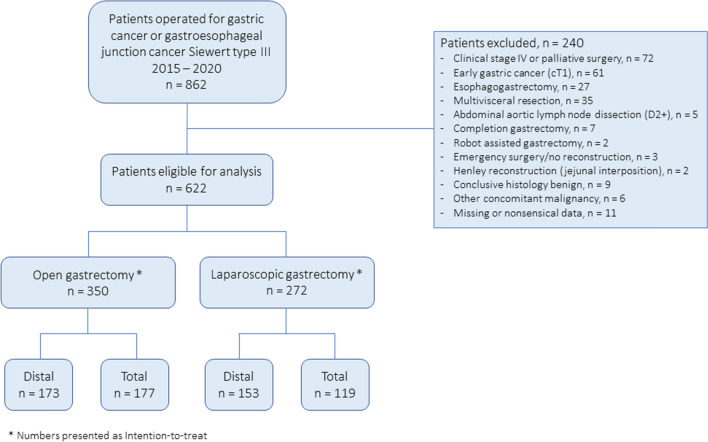
Patients who underwent surgery with curative intent for adenocarcinoma of the stomach or gastroesophageal junction Siewert type III from 2015 to 2020 were identified, and 622 patients with cT2-4aN0-3M0 tumors were included. The impact of surgical approach on short-term outcomes was assessed using multivariable logistic regression. Long-term survival was compared using multivariable Cox regression.
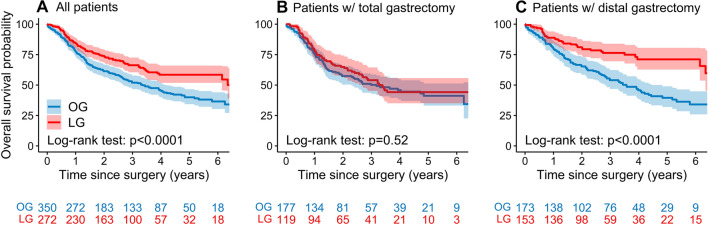
In total, 350 patients underwent open and 272 laparoscopic gastrectomy, of which 12.9% were converted to open surgery. The groups were similar regarding distribution of clinical disease stage (27.6% stage I, 46.0% stage II, and 26.4% stage III). Neoadjuvant chemotherapy was administered to 52.7% of the patients. There was no difference in the rate of postoperative complications, but laparoscopic approach was associated with lower 90 day mortality (1.8 vs 4.9%, p = 0.043). The median number of resected lymph nodes was higher after laparoscopic surgery (32 vs 26, p < 0.001), while no difference was found in the rate of tumor-free resection margins. Better overall survival was observed after laparoscopic gastrectomy (HR 0.63, p < 0.001).
Laparoscopic gastrectomy can be safely preformed for advanced gastric cancer and is associated with improved overall survival compared to open surgery.
腹腔镜胃切除术越来越多地用于治疗局部进展期胃癌,但人们仍然担心与开放胃切除术相比是否能获得类似的结果,尤其是在西方人群中。本研究基于瑞典食管和胃癌登记处的数据,比较了腹腔镜与开放胃切除术治疗 Siewert Ⅲ型胃食管结合部腺癌患者的短期术后、肿瘤学和生存结果。
确定了 2015 年至 2020 年间接受根治性手术治疗胃或胃食管结合部腺癌的患者,并纳入了 622 例 cT2-4aN0-3M0 肿瘤患者。使用多变量逻辑回归评估手术方式对短期结果的影响。使用多变量 Cox 回归比较长期生存。
共有 350 例患者接受了开放手术,272 例患者接受了腹腔镜手术,其中 12.9%的患者转为开放手术。两组临床疾病分期分布相似(Ⅰ期 27.6%,Ⅱ期 46.0%,Ⅲ期 26.4%)。52.7%的患者接受了新辅助化疗。术后并发症发生率无差异,但腹腔镜手术 90 天死亡率较低(1.8% vs 4.9%,p=0.043)。腹腔镜手术切除的淋巴结数量中位数较高(32 个 vs 26 个,p<0.001),但无肿瘤切缘率无差异。腹腔镜胃切除术的总生存率更好(HR 0.63,p<0.001)。
腹腔镜胃切除术可安全用于治疗进展期胃癌,与开放手术相比,腹腔镜胃切除术总体生存率提高。