Division of Digestive and Liver Diseases, University of Texas Southwestern Medical Center, Dallas, Texas.
Department of Gastroenterology and Hepatology, Kindai University Faculty of Medicine, Osaka Japan.
Clin Gastroenterol Hepatol. 2023 Jul;21(8):2135-2149. doi: 10.1016/j.cgh.2023.01.039. Epub 2023 Feb 20.
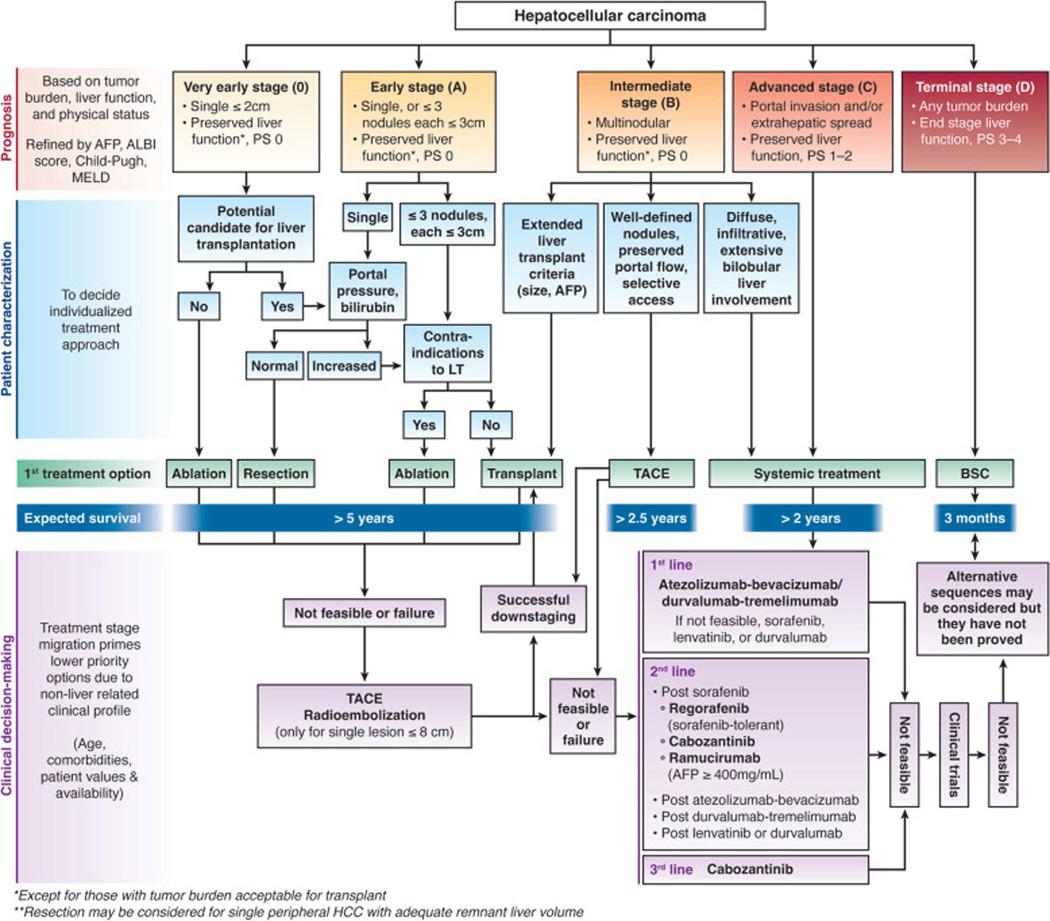
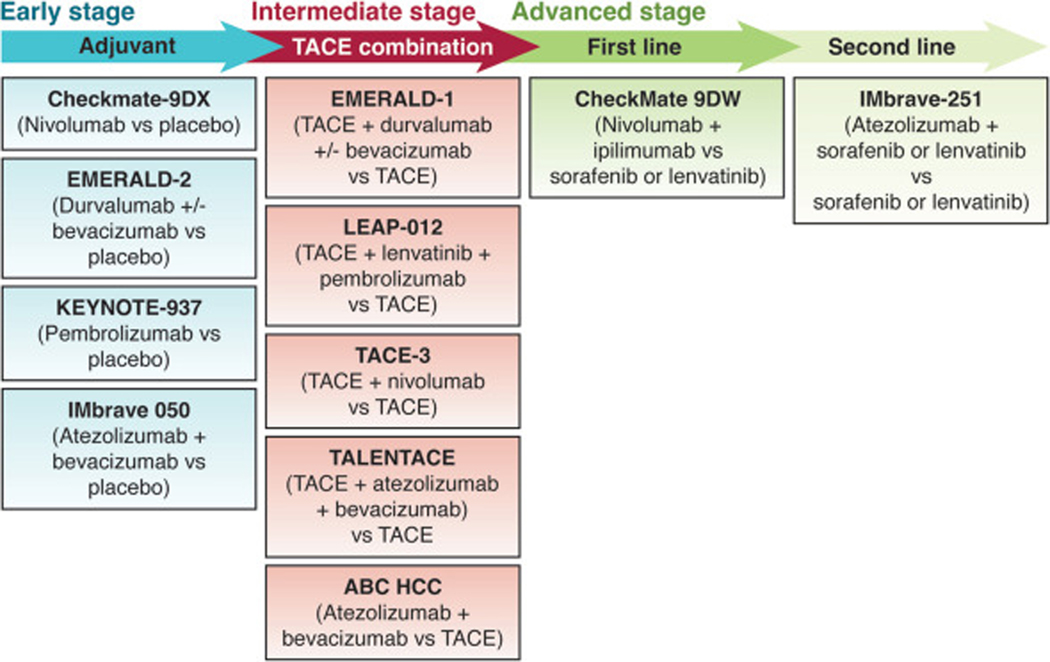
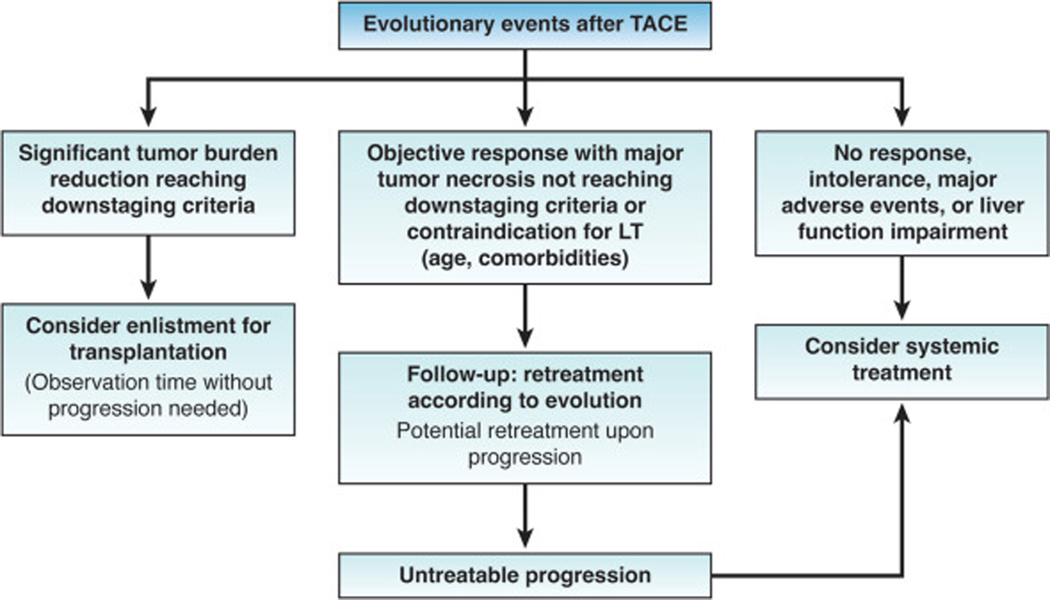
Several breakthroughs in hepatocellular carcinoma (HCC) therapy across tumor stages provide hope to improve its dismal prognosis. Although surgical and local ablative therapies have few significant changes in technique, an improved understanding of tumor biology has facilitated increase numbers of patients who are now eligible to undergo curative-intent procedures. Most notably, acceptable post-transplant outcomes can be achieved in well selected patients whose tumors are downstaged into Milan Criteria. Adjuvant therapy in patients at high risk of recurrence also significantly improves recurrence-free survival after resection or ablation. For patients with liver-localized disease who are not eligible for curative-intent procedures, transarterial chemoembolization (TACE) was historically the treatment modality of choice, regardless of tumor burden; however, there is now increased recognition of patients who are "TACE unsuitable" and may be better treated with systemic therapy. The greatest evolution in HCC treatment options has occurred with systemic therapy, where several new agents are now available in the first- and second-line setting, including immune checkpoint inhibitor combinations. Objective responses are observed in approximately 30% of patients and median survival is approaching 2 years. The availability of immune checkpoint inhibitors has renewed interest in combination therapies for earlier tumor stages, with several phase III trials ongoing. Considering increasing complexities of HCC care, requiring decisions between therapies delivered by different providers, multidisciplinary care is critical and is associated with improved clinical outcomes. In this review, we detail major breakthroughs in HCC therapy, how these breakthroughs can be applied in clinical practice, and remaining areas in need of further research.
在肝癌 (HCC) 治疗的各个肿瘤阶段都取得了一些突破,这为改善其惨淡的预后带来了希望。尽管手术和局部消融治疗在技术上没有太大变化,但对肿瘤生物学的深入了解使得更多符合条件的患者能够接受根治性手术。最值得注意的是,在肿瘤降期符合米兰标准的精选患者中,可以获得可接受的移植后结果。对于有高复发风险的患者进行辅助治疗,也可以显著改善切除或消融后的无复发生存率。对于不适合根治性手术的局限性肝内疾病患者,经动脉化疗栓塞 (TACE) 一直是首选的治疗方式,无论肿瘤负荷如何;然而,现在越来越多的患者被认为是“不适合 TACE”,可能需要接受系统治疗。HCC 治疗选择的最大进展出现在系统治疗方面,目前在一线和二线治疗中已经有几种新的药物可供使用,包括免疫检查点抑制剂联合用药。大约 30%的患者观察到客观缓解,中位生存期接近 2 年。免疫检查点抑制剂的出现重新激发了对早期肿瘤阶段联合治疗的兴趣,目前正在进行多项 III 期试验。考虑到 HCC 治疗的复杂性不断增加,需要在不同提供者提供的治疗方法之间做出决策,多学科护理至关重要,并且与改善临床结果相关。在这篇综述中,我们详细介绍了 HCC 治疗的主要突破,以及这些突破如何在临床实践中应用,以及仍需要进一步研究的领域。