Division of Gastroenterology, Department of Medicine, Kurume University School of Medicine, Kurume City, Fukuoka, Japan.
Liver Cancer Research Division, Research Center for Innovative Cancer Therapy, Kurume University, Kurume City, Fukuoka, Japan.
Cancer Commun (Lond). 2023 Apr;43(4):415-434. doi: 10.1002/cac2.12411. Epub 2023 Feb 24.
Antiangiogenic tyrosine kinase inhibitors (TKIs) provide one of the few therapeutic options for effective treatment of hepatocellular carcinoma (HCC). However, patients with HCC often develop resistance toward antiangiogenic TKIs, and the underlying mechanisms are not understood. The aim of this study was to determine the mechanisms underlying antiangiogenic TKI resistance in HCC.
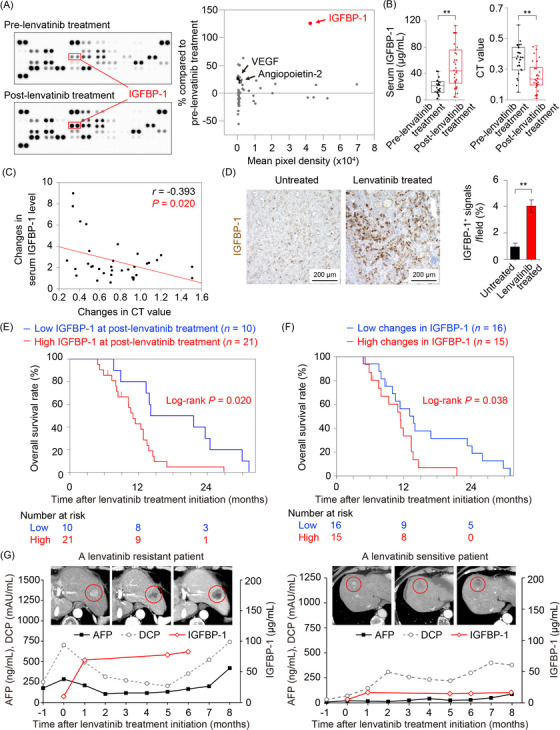
We used an unbiased proteomic approach to define proteins that were responsible for the resistance to antiangiogenic TKIs in HCC patients. We evaluated the prognosis, therapeutic response, and serum insulin-like growth factor-binding protein-1 (IGFBP-1) levels of 31 lenvatinib-treated HCC patients. Based on the array of results, a retrospective clinical study and preclinical experiments using mouse and human hepatoma cells were conducted. Additionally, in vivo genetic and pharmacological gain- and loss-of-function experiments were performed.
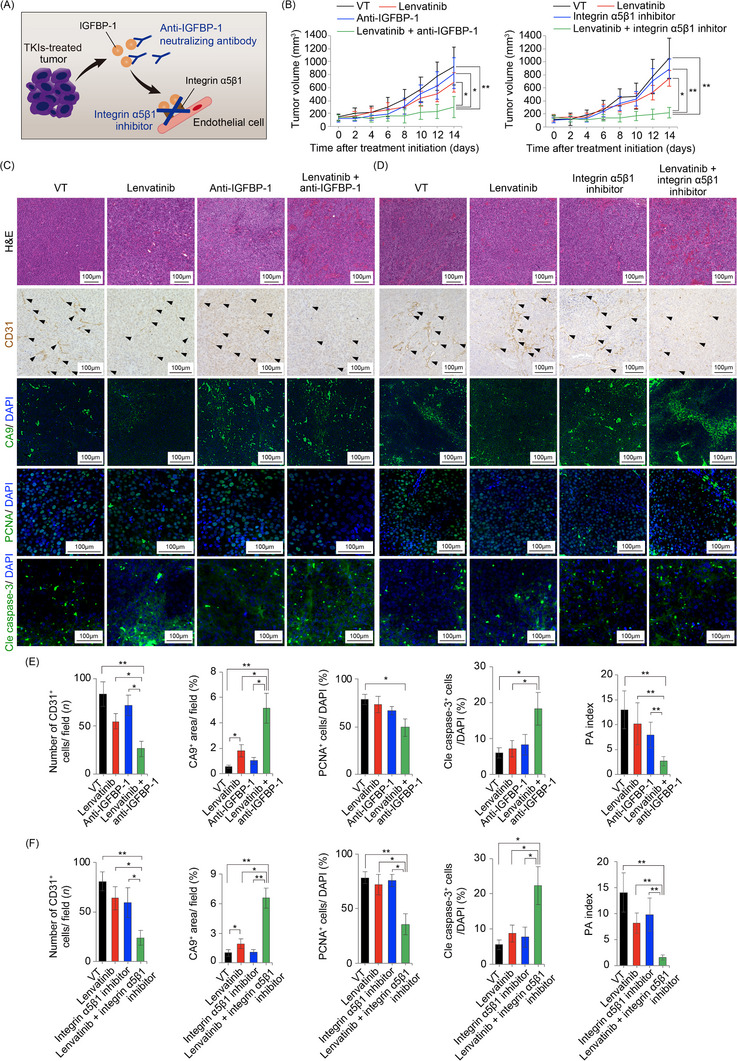
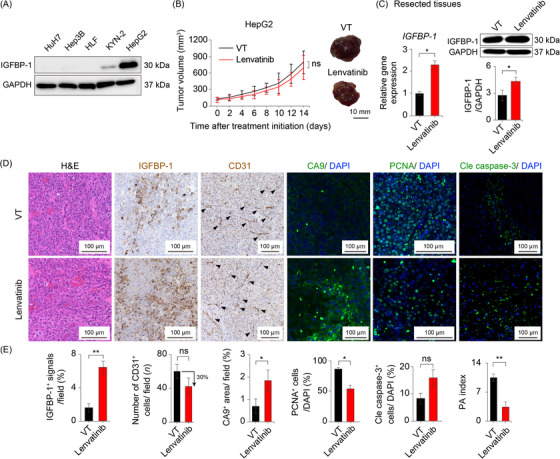
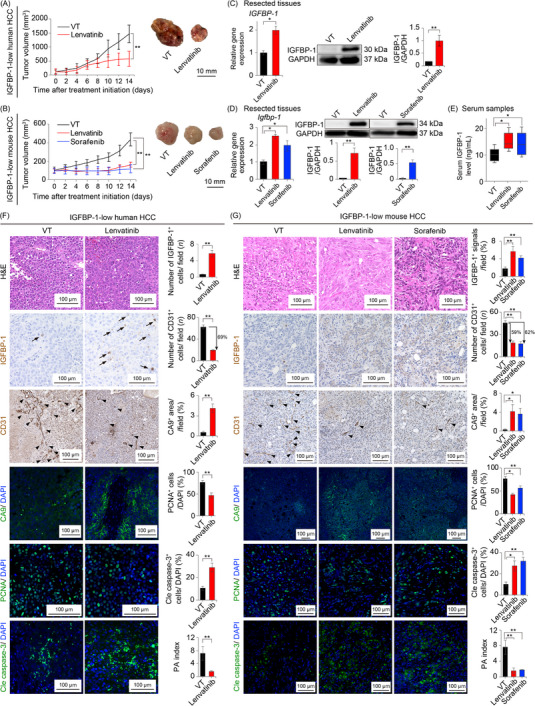
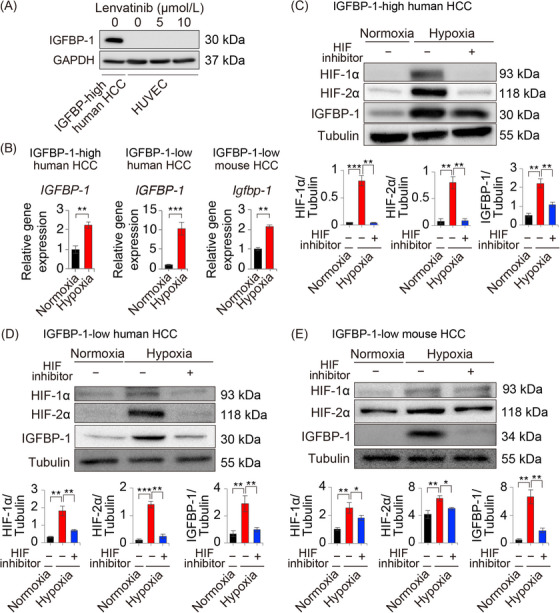
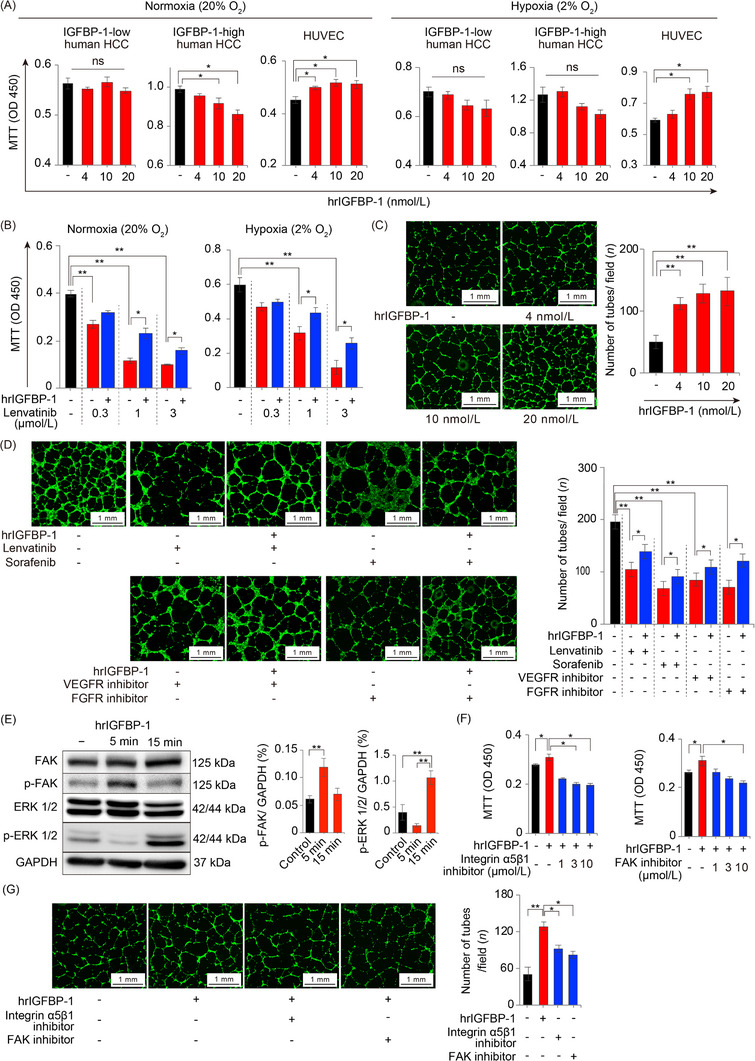
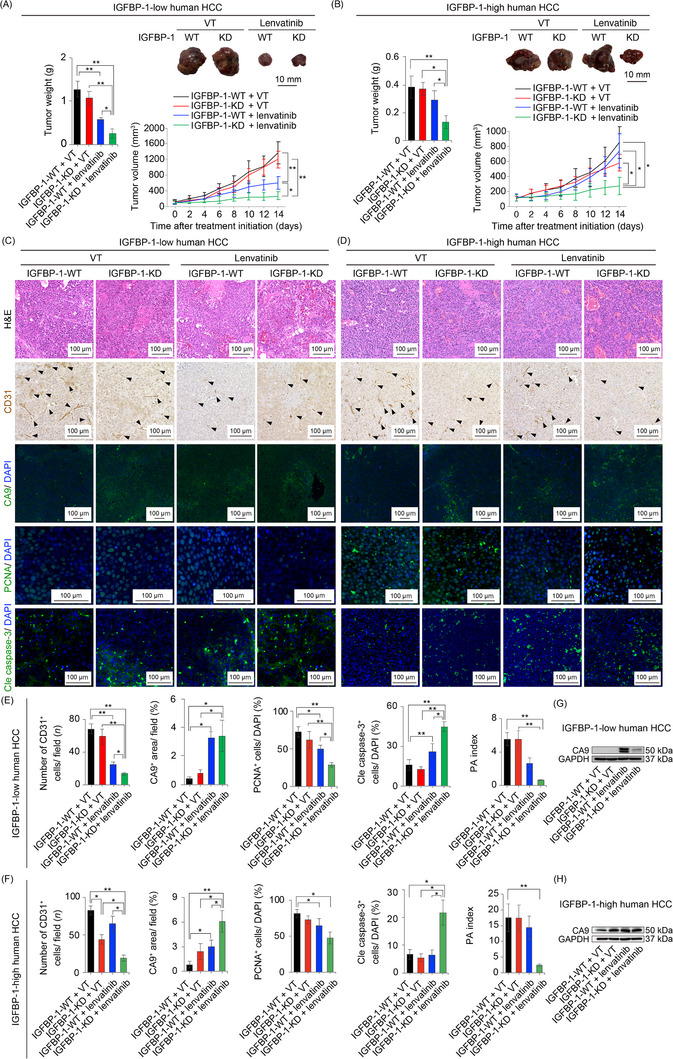
In the patient cohort, IGFBP-1 was identified as the signaling molecule with the highest expression that was inversely associated with overall survival. Mechanistically, antiangiogenic TKI treatment markedly elevated tumor IGFBP-1 levels via the hypoxia-hypoxia inducible factor signaling. IGFBP-1 stimulated angiogenesis through activation of the integrin α5β1-focal adhesion kinase pathway. Consequently, loss of IGFBP-1 and integrin α5β1 by genetic and pharmacological approaches re-sensitized HCC to lenvatinib treatment.
Together, our data shed light on mechanisms underlying acquired resistance of HCC to antiangiogenic TKIs. Antiangiogenic TKIs induced an increase of tumor IGFBP-1, which promoted angiogenesis through activating the IGFBP-1-integrin α5β1 pathway. These data bolster the application of a new therapeutic concept by combining antiangiogenic TKIs with IGFBP-1 inhibitors.
血管生成酪氨酸激酶抑制剂(TKI)为治疗肝细胞癌(HCC)提供了为数不多的有效治疗选择之一。然而,HCC 患者经常对血管生成 TKI 产生耐药性,其潜在机制尚不清楚。本研究旨在确定 HCC 患者对血管生成 TKI 耐药的机制。
我们使用无偏倚的蛋白质组学方法来确定导致 HCC 患者对血管生成 TKI 耐药的蛋白。我们评估了 31 名接受仑伐替尼治疗的 HCC 患者的预后、治疗反应和血清胰岛素样生长因子结合蛋白-1(IGFBP-1)水平。根据结果数组,进行了回顾性临床研究和使用小鼠和人肝癌细胞的临床前实验。此外,还进行了体内遗传和药理学增益和损失功能实验。
在患者队列中,IGFBP-1 被确定为表达最高且与总生存期呈负相关的信号分子。从机制上讲,血管生成 TKI 治疗通过缺氧-缺氧诱导因子信号显著增加肿瘤 IGFBP-1 水平。IGFBP-1 通过激活整合素α5β1-粘着斑激酶途径刺激血管生成。因此,通过遗传和药理学方法丧失 IGFBP-1 和整合素α5β1 可使 HCC 重新对仑伐替尼治疗敏感。
总的来说,我们的数据阐明了 HCC 对血管生成 TKI 获得性耐药的机制。血管生成 TKI 诱导肿瘤 IGFBP-1 增加,通过激活 IGFBP-1-整合素α5β1 途径促进血管生成。这些数据支持通过将血管生成 TKI 与 IGFBP-1 抑制剂联合应用来提出新的治疗概念。