Department of Policlinics, Centre for Primary Care and Public Health (Unisanté), Lausanne, Switzerland.
Department of Epidemiology and Health Systems, Centre for Primary Care and Public Health (Unisanté), Lausanne, Switzerland.
PLoS One. 2023 Feb 24;18(2):e0282150. doi: 10.1371/journal.pone.0282150. eCollection 2023.
Nasopharyngeal antigen Rapid Diagnostic Tests (RDTs), saliva RT-PCR and nasopharyngeal (NP) RT-PCR have shown different performance characteristics to detect patients infected by SARS-CoV-2, according to the viral load (VL)-and thus transmissibility.
In October 2020, we conducted a prospective trial involving patients presenting at testing centres with symptoms of COVID-19. We compared detection rates and performance of RDT, saliva PCR and nasopharyngeal (NP) PCR, according to VL and symptoms duration.
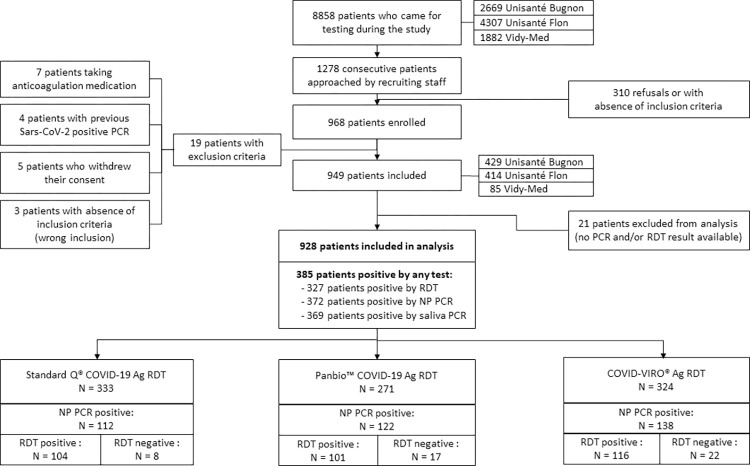
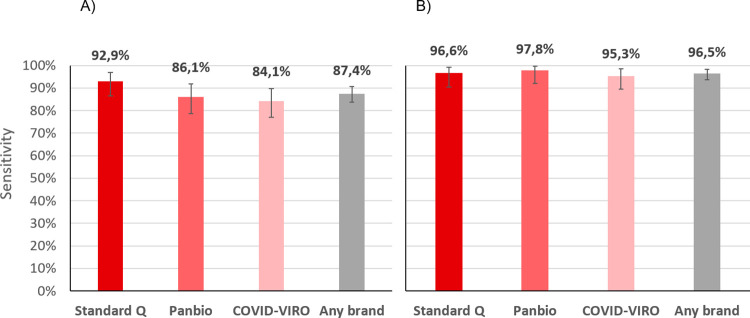
Out of 949 patients enrolled, 928 patients had all three tests performed. Detection rates were 35.2% (95%CI 32.2-38.4%) by RDT, 39.8% (36.6-43.0%) by saliva PCR, 40.1% (36.9-43.3%) by NP PCR, and 41.5% (38.3-44.7%) by any test. For those with viral loads (VL) ≥106 copies/ml, detection rates were 30.3% (27.3-33.3), 31.4% (28.4-34.5), 31.5% (28.5-34.6), and 31.6% (28.6-34.7%) respectively. Sensitivity of RDT compared to NP PCR was 87.4% (83.6-90.6%) for all positive patients, 94.5% (91.5-96.7%) for those with VL≥105 and 96.5% (93.6-98.3%) for those with VL≥106. Sensitivity of STANDARD-Q®, Panbio™ and COVID-VIRO® Ag tests were 92.9% (86.4-96.9%), 86.1% (78.6-91.7%) and 84.1% (76.9-89.7%), respectively. For those with VL≥106, sensitivity was 96.6% (90.5-99.3%), 97.8% (92.1-99.7%) and 95.3% (89.4-98.5%) respectively. No patient with VL<104 was detected by RDT. Specificity of RDT was 100% (99.3-100%) compared to any PCR. RDT sensitivity was similar <4 days (87.8%, 83.5-91.3%) and ≥4 days (85.7%, 75.9-92.6%) after symptoms onset (p = 0.6). Sensitivity of saliva and NP PCR were 95.7% (93.1-97.5%) and 96.5% (94.1-98.1%), respectively, compared to the other PCR.
RDT results allow rapid identification of COVID cases with immediate isolation of most contagious individuals. RDT can thus be a game changer both in ambulatory care and community testing aimed at stopping transmission chains, and even more so in resource-constrained settings thanks to its very low price. When PCR is performed, saliva could replace NP swabbing.
ClinicalTrial.gov Identifier: NCT04613310 (03/11/2020).
根据病毒载量(VL)-因此也具有传染性,鼻咽抗原快速诊断检测(RDT)、唾液 RT-PCR 和鼻咽(NP)RT-PCR 检测 SARS-CoV-2 感染患者的表现特征不同。
2020 年 10 月,我们开展了一项前瞻性试验,纳入了在检测中心出现 COVID-19 症状的患者。我们比较了 RDT、唾液 PCR 和鼻咽(NP)PCR 的检测率和性能,根据 VL 和症状持续时间进行比较。
949 名入组患者中,928 名患者进行了所有三种检测。RDT 的检测率为 35.2%(95%CI 32.2-38.4%),唾液 PCR 为 39.8%(36.6-43.0%),NP PCR 为 40.1%(36.9-43.3%),任何一种检测的检测率为 41.5%(38.3-44.7%)。对于 VL≥106 拷贝/ml 的患者,检测率分别为 30.3%(27.3-33.3)、31.4%(28.4-34.5)、31.5%(28.5-34.6)和 31.6%(28.6-34.7%)。RDT 与 NP PCR 相比,所有阳性患者的灵敏度分别为 87.4%(83.6-90.6%),VL≥105 的患者灵敏度为 94.5%(91.5-96.7%),VL≥106 的患者灵敏度为 96.5%(93.6-98.3%)。STANDARD-Q®、Panbio™和 COVID-VIRO®Ag 检测的灵敏度分别为 92.9%(86.4-96.9%)、86.1%(78.6-91.7%)和 84.1%(76.9-89.7%)。对于 VL≥106 的患者,灵敏度分别为 96.6%(90.5-99.3%)、97.8%(92.1-99.7%)和 95.3%(89.4-98.5%)。RDT 未能检测到 VL<104 的患者。与任何 PCR 相比,RDT 的特异性为 100%(99.3-100%)。RDT 的灵敏度在症状出现后<4 天(87.8%,83.5-91.3%)和≥4 天(85.7%,75.9-92.6%)时相似(p=0.6)。与其他 PCR 相比,唾液和 NP PCR 的灵敏度分别为 95.7%(93.1-97.5%)和 96.5%(94.1-98.1%)。
RDT 结果可以快速识别 COVID 病例,并立即对大多数传染性个体进行隔离。因此,RDT 无论是在门诊护理还是在社区检测中,都可以改变传播链,尤其是在资源有限的情况下,因为它的价格非常低。当进行 PCR 检测时,唾液可以替代鼻咽拭子。
ClinicalTrials.gov 标识符:NCT04613310(2020 年 11 月 3 日)。