Bottoni Edoardo, Mangiameli Giuseppe, Testori Alberto, Piccioni Federico, Giudici Veronica Maria, Voulaz Emanuele, Ruggieri Nadia, Dalla Corte Francesca, Crepaldi Alessandro, Goretti Giulia, Vanni Elena, Pisarra Martina, Cariboni Umberto, Alloisio Marco, Cecconi Maurizio
Division of Thoracic Surgery, IRCCS Humanitas Research Hospital, Via Manzoni 56, Rozzano, 20089 Milan, Italy.
Department of Biomedical Sciences, Humanitas University, Via Rita Levi Montalcini 4, Pieve Emanuele, 20090 Milan, Italy.
Cancers (Basel). 2023 Feb 10;15(4):1146. doi: 10.3390/cancers15041146.
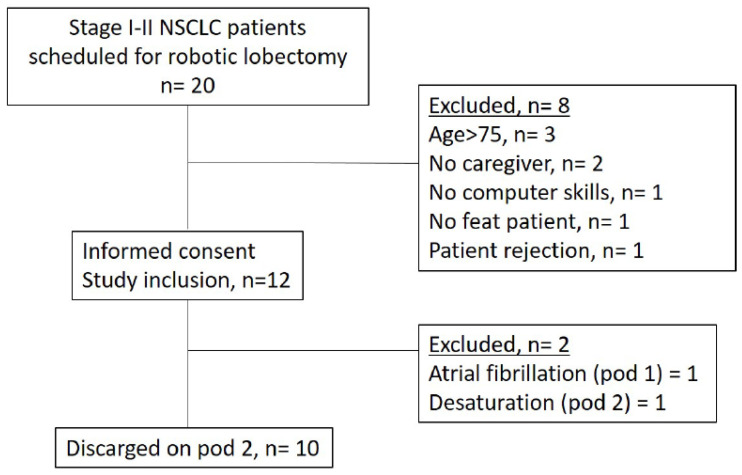
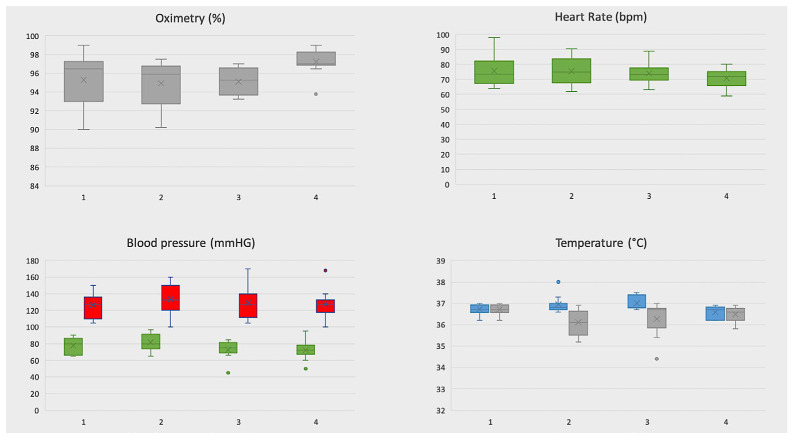
Despite the adoption of enhanced recovery programs, the reported postoperative length of stay after robotic surgery is 4 days even in highly specialized centers. We report preliminary results of a pilot study for a new protocol of early discharge (on day 2) with telehealth home monitoring after robotic lobectomy for lung cancer. All patients with a caregiver were discharged on postoperative day 2 with a telemonitoring device if they satisfied specific discharge criteria. Teleconsultations were scheduled once in the afternoon of post-operative day 2, twice on postoperative day 3, and then once a day until the chest tube removal. Post-discharge vital signs were recorded by patients at least four times daily through the device and were available for consultation by two surgeons through phone application. In case of sudden variation of vital signs or occurrence of adverse events, a direct telephone line was available for patients as well as a protected re-hospitalization path. Primary outcome was the safety evaluated by the occurrence of post-discharge complications and readmissions. Secondary outcome was the evaluation of resources optimization (hospitalization days) maintaining the standard of care. During the study period, twelve patients satisfied all preoperative clinical criteria to be enrolled in our protocol. Two of twelve enrolled patients were successively excluded because they did not satisfy discharge criteria on postoperative day 2. During telehealth home monitoring a total of 27/427 vital-sign measurements violated the threshold in seven patients. Among the threshold violations, only 1 out of 27 was a critical violation and was managed at home. No postoperative complication occurred neither readmission was needed. A mean number of three hospitalization days was avoided and an estimated economic benefit of about EUR 500 for a single patient was obtained if compared with patients submitted to VATS lobectomy in the same period. These preliminary results confirm that adoption of telemonitoring allows, in selected patients, a safe discharge on postoperative day 2 after robotic surgery for early-stage NSCLC. A potential economic benefit could derive from this protocol if this data will be confirmed in larger sample.
尽管采用了强化康复计划,但即使在高度专业化的中心,机器人手术后报告的术后住院时间仍为4天。我们报告了一项初步研究的结果,该研究针对肺癌机器人肺叶切除术后采用远程医疗家庭监测的新早期出院方案(术后第2天出院)。所有有护理人员的患者如果满足特定出院标准,在术后第2天配备远程监测设备出院。术后第2天下午安排一次远程会诊,术后第3天安排两次,然后每天安排一次,直至拔除胸管。出院后患者通过该设备每天至少记录四次生命体征,两位外科医生可通过手机应用程序查阅。如果生命体征突然变化或发生不良事件,患者可拨打直接电话线,还有一条受保护的再次住院途径。主要结局是通过出院后并发症和再入院情况评估安全性。次要结局是评估在维持护理标准的同时优化资源(住院天数)。在研究期间,12名患者满足所有术前临床标准可纳入我们的方案。12名纳入患者中有2名随后被排除,因为他们在术后第2天不满足出院标准。在远程医疗家庭监测期间,427次生命体征测量中有27次超过阈值,涉及7名患者。在超过阈值的情况中,27次中只有1次是严重违规,在家庭中得到处理。未发生术后并发症,也无需再次入院。与同期接受电视辅助胸腔镜肺叶切除术的患者相比,平均避免了三天的住院时间,单例患者估计获得约500欧元的经济效益。这些初步结果证实,对于早期非小细胞肺癌患者,采用远程监测可使其在机器人手术后安全地在术后第2天出院。如果这些数据在更大样本中得到证实,该方案可能会带来潜在的经济效益。