Department of Surgical Oncology, University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands.
Department of Epidemiology, University of Groningen, University Medical Centre Groningen, Groningen, The Netherlands.
Ann Surg Oncol. 2021 Oct;28(11):6512-6522. doi: 10.1245/s10434-021-09707-3. Epub 2021 Feb 27.
Postoperative home monitoring could potentially detect complications early, but evidence in oncogeriatric surgery is scarce. Therefore, we evaluated whether post-discharge physical activity, vital signs, and patient-reported symptoms are related to post-discharge complications and hospital readmissions in older patients undergoing cancer surgery.
In this observational cohort study, we monitored older patients (≥65 years of age) undergoing cancer surgery, for 2 weeks post-discharge using tablet-based applications and connected devices. Outcome measures were post-discharge complications and readmissions; physical activity and patient-reported symptoms over time; and threshold violations for physical activity (step count <1000 steps/day), vital signs (temperature <36°C or >38°C; blood pressure <100/60 mmHg or >150/100 mmHg; heart rate <50 bpm or >100 bpm; weight -5% or +5% of weight at discharge); and patient-reported symptoms (pain score greater than the previous day; presence of dyspnea, vomiting, dizziness, fever).
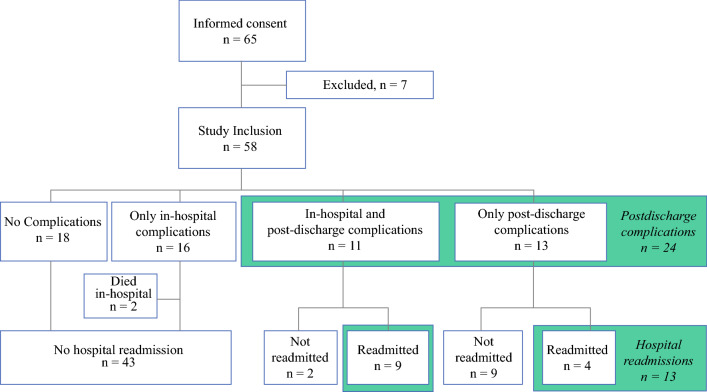
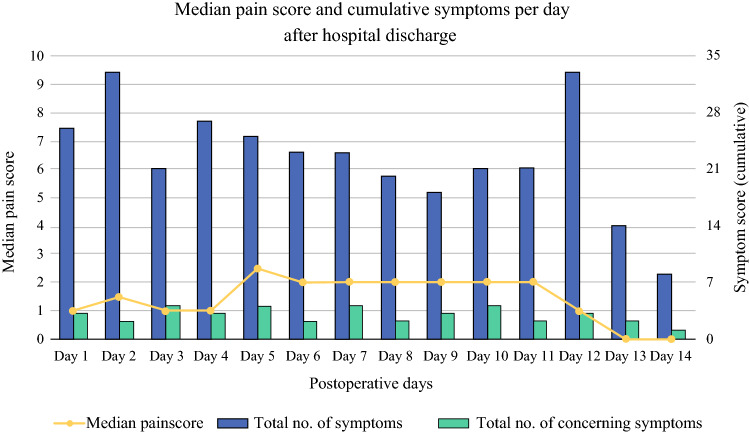
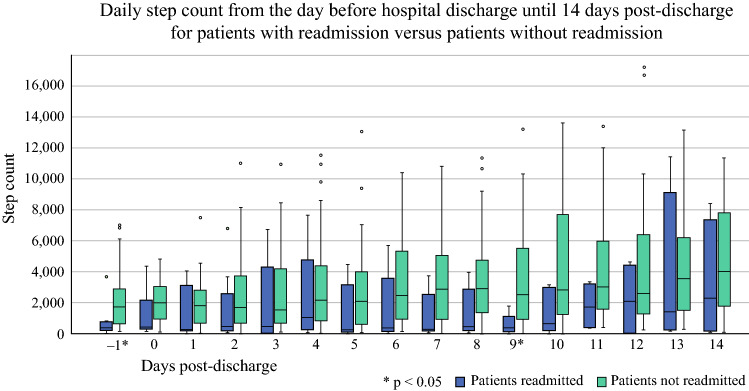
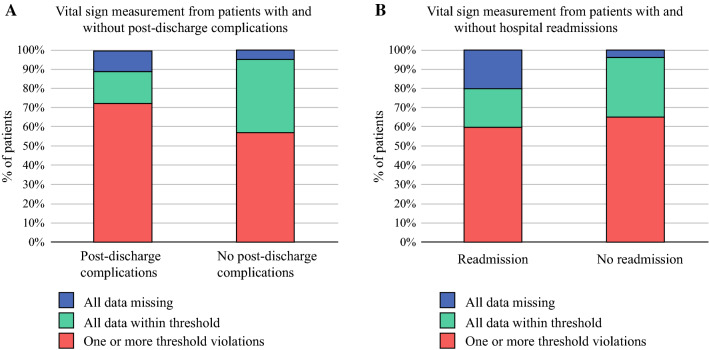
Of 58 patients (mean age 72 years), 24 developed a post-discharge complication and 13 were readmitted. Measured parameters indicated 392 threshold violations out of 5379 measurements (7.3%) in 40 patients, mostly because of physical inactivity. Patients with readmissions had lower physical activity at discharge and at day 9 after discharge and violated a physical activity threshold more often. Patients with post-discharge complications had a higher median pain score compared with patients without these adverse events. No differences in threshold violations of other parameters were observed between patients with and without post-discharge complications and readmissions.
Our results show the potential of telemonitoring older patients after cancer surgery but confirm that detecting post-discharge complications is complex and multifactorial.
术后居家监测有可能早期发现并发症,但在老年肿瘤患者手术中相关证据有限。因此,我们评估了癌症手术后出院的老年患者的身体活动、生命体征和患者报告的症状与出院后并发症和再入院之间的关系。
在这项观察性队列研究中,我们使用基于平板电脑的应用程序和连接设备,对接受癌症手术的老年患者(≥65 岁)进行出院后 2 周的监测。结局指标为出院后并发症和再入院;随时间推移的身体活动和患者报告的症状;以及身体活动(步数<1000 步/天)、生命体征(体温<36°C 或>38°C;血压<100/60mmHg 或>150/100mmHg;心率<50bpm 或>100bpm;体重比出院时下降 5%或增加 5%)和患者报告的症状(疼痛评分比前一天高;存在呼吸困难、呕吐、头晕、发热)的阈值违规。
在 58 例患者(平均年龄 72 岁)中,24 例发生出院后并发症,13 例再入院。在 40 例患者中,5379 次测量中有 392 次(7.3%)出现测量参数的阈值违规,主要是由于身体不活动。再入院患者出院时和出院后第 9 天的身体活动量较低,且违反身体活动阈值的情况更为常见。与无这些不良事件的患者相比,发生出院后并发症的患者的中位疼痛评分更高。未观察到有出院后并发症和再入院患者的其他参数的阈值违规之间存在差异。
我们的结果表明,对老年肿瘤患者手术后进行远程监测具有潜力,但也证实了检测出院后并发症是复杂和多因素的。