Sessa Francesco, Nicoletti Rossella, Pecoraro Alessio, Polverino Paolo, Rivetti Anna, Conte Francesco Lupo, Lo Re Mattia, Belmonte Mario, Alberti Andrea, Dibilio Edoardo, Gallo Maria Lucia, Manera Alekseja, Gacci Mauro, Sebastianelli Arcangelo, Vignolini Graziano, Serni Sergio, Campi Riccardo, Li Marzi Vincenzo
Unit of Urological Robotic Surgery and Renal Transplantation, Careggi Hospital, University of Florence, 50100 Florence, Italy.
Department of Experimental and Clinical Medicine, University of Florence, 50100 Florence, Italy.
J Clin Med. 2023 Feb 8;12(4):1358. doi: 10.3390/jcm12041358.
The aim of our study is to evaluate the prevalence and predictive factors of short- (30 d) and mid-term continence in a contemporary cohort of patients treated with robotic-assisted laparoscopic prostatectomy (RALP) without any posterior or anterior reconstruction at our referral academic center.
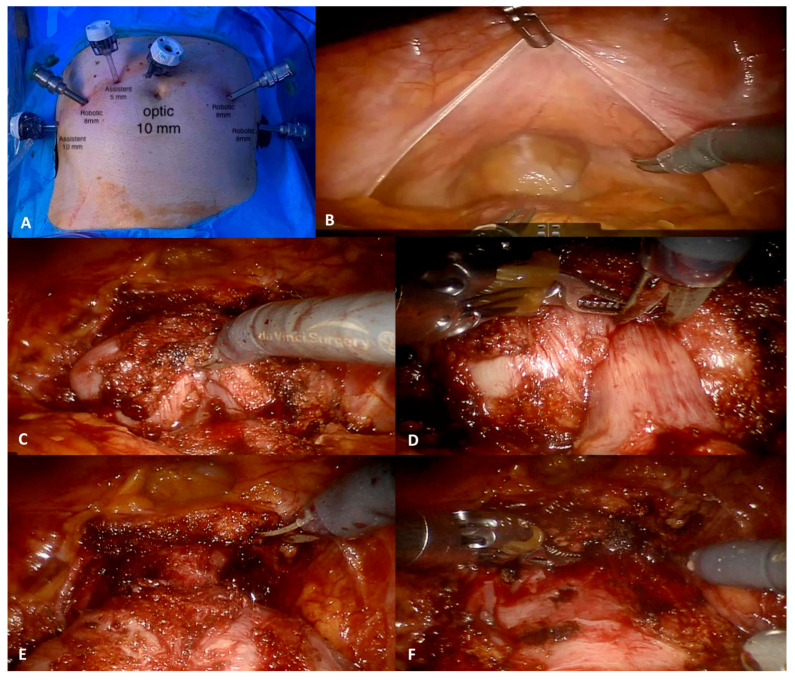
Data from patients undergoing RALP between January 2017 and March 2021 were prospectively collected. RALP was performed by three highly experienced surgeons following the principles of the Montsouris technique, with a bladder-neck-sparing intent and maximal preservation of the membranous urethra (if oncologically safe) without any anterior/posterior reconstruction. (Self-assessed urinary incontinence (UI) was defined as the need of one or more pads per die (excluding the need for a safety pad/die. Univariable and multivariable logistic regression analysis was used to assess the independent predictors of early incontinence among routinely collected patient- and tumor-related variables).
A total of 925 patients were included; of these, 353 underwent RALP (38.2%) without nerve-sparing intent. The median patient age and BMI were 68 years (IQR 63-72) and 26 (IQR 24.0-28.0), respectively. Overall, 159 patients (17.2%) reported early (30 d) incontinence. In multivariable analysis adjusting for patient- and tumor-related features, a non-nerve-sparing procedure (OR: 1.57 [95% CI: 1.03-2.59], = 0.035) was independently associated with the risk of urinary incontinence in the short-term period, while the absence of cardiovascular diseases before surgery (OR: 0.46 [95% CI: 0.320.67], ≤ 0.01) was a protective factor for this outcome. At a median follow-up of 17 months (IQR 10-24), 94.5% of patients reported to be continent.
In experienced hands, most patients fully recover urinary continence after RALP at mid-term follow-up. On the contrary, the proportion of patients who reported early incontinence in our series was modest but not negligible. The implementation of surgical techniques advocating anterior and/or posterior fascial reconstruction might improve the early continence rate in candidates for RALP.
我们研究的目的是评估在我们转诊学术中心接受机器人辅助腹腔镜前列腺切除术(RALP)且未进行任何前后部重建的当代患者队列中,短期(30天)和中期尿失禁的患病率及预测因素。
前瞻性收集2017年1月至2021年3月期间接受RALP患者的数据。RALP由三位经验丰富的外科医生按照蒙苏里技术原则进行,旨在保留膀胱颈并最大程度保留膜性尿道(如果肿瘤学上安全),不进行任何前后部重建。(自我评估的尿失禁(UI)定义为每天需要一个或多个尿垫(不包括需要安全尿垫/天)。使用单变量和多变量逻辑回归分析来评估常规收集的患者和肿瘤相关变量中早期尿失禁的独立预测因素)。
共纳入925例患者;其中,353例(38.2%)接受了非保留神经的RALP。患者的中位年龄和BMI分别为68岁(IQR 63 - 72)和26(IQR 24.0 - 28.0)。总体而言,159例患者(17.2%)报告早期(30天)尿失禁。在针对患者和肿瘤相关特征进行调整的多变量分析中,非保留神经手术(OR:1.57 [95% CI:1.03 - 2.59],P = 0.035)与短期尿失禁风险独立相关,而术前无心血管疾病(OR:0.46 [95% CI:0.32 - 0.67],P ≤ 0.01)是该结果的保护因素。中位随访17个月(IQR 10 - 24)时,94.5%的患者报告为尿控良好。
在经验丰富的医生手中,大多数患者在中期随访时RALP后能完全恢复尿控。相反,我们系列中报告早期尿失禁的患者比例虽小但不可忽视。倡导进行前部和/或后部筋膜重建的手术技术的实施可能会提高RALP候选患者的早期尿控率。