Institute of Social and Preventive Medicine, University of Bern, Bern, Switzerland.
Emergency Department, Inselspital, Bern University Hospital, University of Bern, Freiburgstrasse 16C, 3010, Bern, Switzerland.
Eur J Epidemiol. 2023 Apr;38(4):355-372. doi: 10.1007/s10654-023-00973-x. Epub 2023 Feb 25.
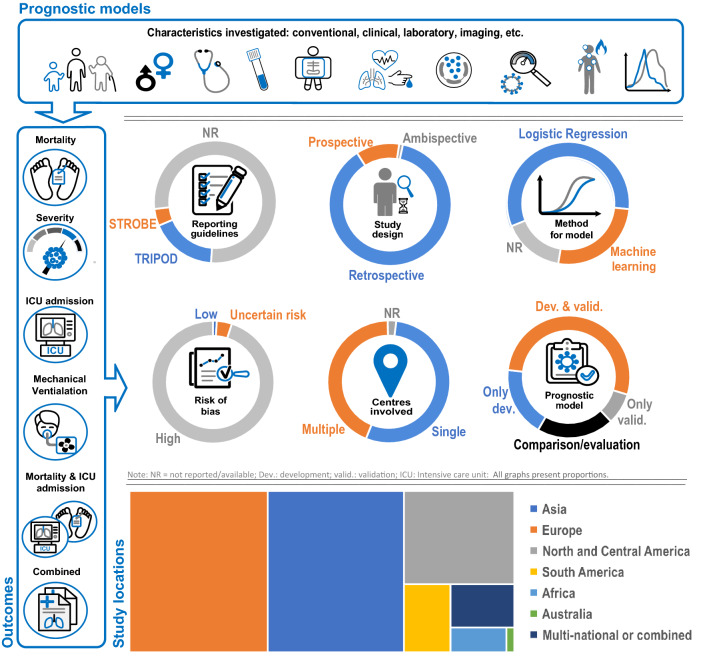
Current evidence on COVID-19 prognostic models is inconsistent and clinical applicability remains controversial. We performed a systematic review to summarize and critically appraise the available studies that have developed, assessed and/or validated prognostic models of COVID-19 predicting health outcomes. We searched six bibliographic databases to identify published articles that investigated univariable and multivariable prognostic models predicting adverse outcomes in adult COVID-19 patients, including intensive care unit (ICU) admission, intubation, high-flow nasal therapy (HFNT), extracorporeal membrane oxygenation (ECMO) and mortality. We identified and assessed 314 eligible articles from more than 40 countries, with 152 of these studies presenting mortality, 66 progression to severe or critical illness, 35 mortality and ICU admission combined, 17 ICU admission only, while the remaining 44 studies reported prediction models for mechanical ventilation (MV) or a combination of multiple outcomes. The sample size of included studies varied from 11 to 7,704,171 participants, with a mean age ranging from 18 to 93 years. There were 353 prognostic models investigated, with area under the curve (AUC) ranging from 0.44 to 0.99. A great proportion of studies (61.5%, 193 out of 314) performed internal or external validation or replication. In 312 (99.4%) studies, prognostic models were reported to be at high risk of bias due to uncertainties and challenges surrounding methodological rigor, sampling, handling of missing data, failure to deal with overfitting and heterogeneous definitions of COVID-19 and severity outcomes. While several clinical prognostic models for COVID-19 have been described in the literature, they are limited in generalizability and/or applicability due to deficiencies in addressing fundamental statistical and methodological concerns. Future large, multi-centric and well-designed prognostic prospective studies are needed to clarify remaining uncertainties.
目前关于 COVID-19 预后模型的证据不一致,临床适用性仍存在争议。我们进行了系统评价,以总结和批判性评估已经开发、评估和/或验证 COVID-19 预后模型以预测健康结果的现有研究。我们搜索了六个文献数据库,以确定调查预测成人 COVID-19 患者不良结局(包括入住重症监护病房(ICU)、插管、高流量鼻治疗(HFNT)、体外膜氧合(ECMO)和死亡)的单变量和多变量预后模型的已发表文章。我们从 40 多个国家中确定并评估了 314 篇合格文章,其中 152 篇报告了死亡率,66 篇报告了进展为严重或危重症,35 篇报告了死亡率和 ICU 入住率,17 篇仅报告了 ICU 入住率,而其余 44 篇报告了机械通气(MV)或多种结局的预测模型。纳入研究的样本量从 11 到 7704171 名参与者不等,平均年龄从 18 到 93 岁不等。研究共探讨了 353 个预后模型,曲线下面积(AUC)从 0.44 到 0.99 不等。很大一部分研究(61.5%,314 篇中的 193 篇)进行了内部或外部验证或复制。在 312 项(99.4%)研究中,由于方法学严谨性、采样、缺失数据处理、未能解决过度拟合以及 COVID-19 和严重程度结局的定义不统一等方面存在不确定性和挑战,预后模型被报告存在高偏倚风险。尽管文献中已经描述了几种 COVID-19 的临床预后模型,但由于在解决基本统计和方法学问题方面存在缺陷,它们的通用性和/或适用性有限。需要进行未来的大型、多中心和精心设计的预后前瞻性研究,以澄清剩余的不确定性。