Xu Yuxuan, Lin Zhihui, Zhu Chenxi, Song Dongyan, Wu Bosen, Ji Kangting, Li Jin
Department of Cardiology, Key Laboratory of Panvascular Diseases of Wenzhou, The Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University, Wenzhou, 325027, People's Republic of China.
J Inflamm Res. 2023 Feb 18;16:691-700. doi: 10.2147/JIR.S394536. eCollection 2023.
The present study aimed to evaluate the relationship between all-cause mortality and the neutrophil percentage-to-albumin ratio (NPAR) in patients with atrial fibrillation (AF).
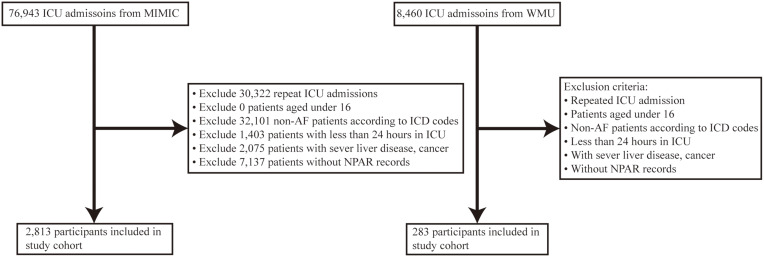
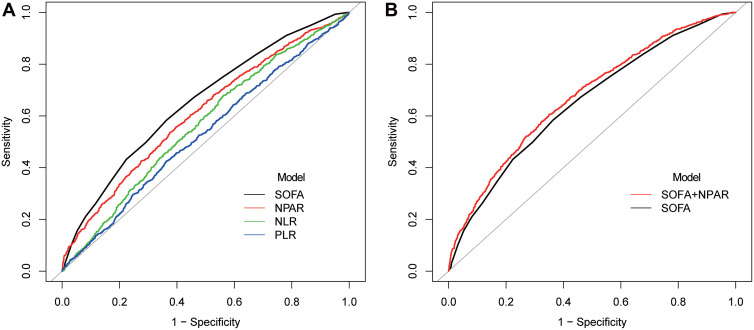
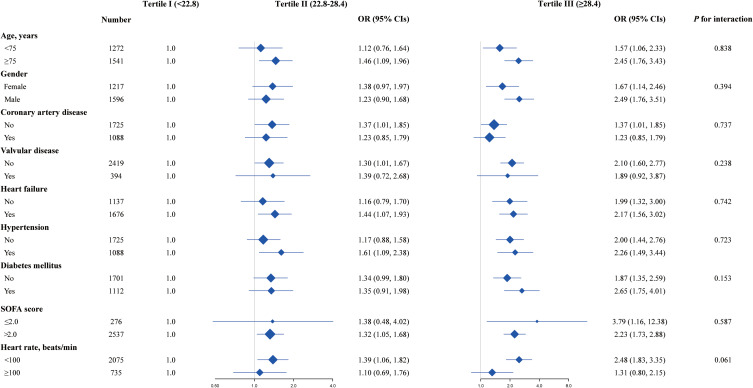
We obtained clinical information from patients with AF from the Medical Information Mart for Intensive Care-IV version 2.0 (MIMIC-IV) database and the Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University (WMU). The clinical endpoints were all-cause death measured at 30-day, 90-day, and one-year intervals. For endpoints associated with the NPAR, logistic regression models were used to calculate odds ratios (OR) with 95% confidence intervals (CI). Receiver operating characteristic (ROC) curves and area under the curve (AUC) were developed to compare the ability of different inflammatory biomarkers to predict 90-day mortality in patients with AF.
Higher NPAR was associated with a higher risk of 30-day (OR 2.08, 95% CI 1.58-2.75), 90-day (OR 2.07, 95% CI 1.61-2.67), and one-year mortality (OR 1.60, 95% CI 1.26-2.04) in patients with AF in 2813 patients from MIMIC-IV. The predictive performance of NPAR (AUC = 0.609) for 90-day mortality was better than that of neutrophil-to-lymphocyte ratio (NLR) (AUC = 0.565, P < 0.001), and platelet-to-lymphocyte ratio (PLR) (AUC = 0.528, P < 0.001). When NPAR and sequential organ failure assessment (SOFA) were combined, the AUC increased from 0.609 to 0.674 (P < 0.001). Higher NPAR was associated with a higher risk of 30-day mortality (OR 2.54, 95% CI 1.02-6.30) and 90-day mortality (OR 2.76, 95% CI 1.09-7.01) in 283 patients from WMU.
An increased 30-day, 90-day, and one-year mortality risk among patients with AF were linked to a higher NPAR in MIMIC-IV. NPAR was thought to be a good predictor of 90-day all-cause mortality. Higher NPAR was associated with a higher risk of 30-day and 90-day mortality in WMU.
本研究旨在评估心房颤动(AF)患者全因死亡率与中性粒细胞百分比与白蛋白比值(NPAR)之间的关系。
我们从重症监护医学信息数据库第四版2.0(MIMIC-IV)以及温州医科大学附属第二医院和育英儿童医院获取了AF患者的临床信息。临床终点为在30天、90天和1年时间间隔测量的全因死亡。对于与NPAR相关的终点,使用逻辑回归模型计算比值比(OR)及95%置信区间(CI)。绘制受试者工作特征(ROC)曲线及曲线下面积(AUC),以比较不同炎症生物标志物预测AF患者90天死亡率的能力。
在MIMIC-IV的2813例AF患者中,较高的NPAR与30天(OR 2.08,95%CI 1.58 - 2.75)、90天(OR 2.07,95%CI 1.61 - 2.67)和1年死亡率(OR 1.60,CI 1.26 - 2.04)风险较高相关。NPAR对90天死亡率的预测性能(AUC = 0.609)优于中性粒细胞与淋巴细胞比值(NLR)(AUC = 0.565,P < 0.001)和血小板与淋巴细胞比值(PLR)(AUC = 0.528,P < 0.001)。当将NPAR与序贯器官衰竭评估(SOFA)相结合时,AUC从0.609增加至0.674(P < 0.001)。在温州医科大学附属第二医院的283例患者中,较高的NPAR与较高的30天死亡率(OR 2.54,95%CI 1.02 - 6.30)和90天死亡率(OR 2.76,95%CI 1.09 - 7.01)风险相关。
在MIMIC-IV中AF患者30天、90天和1年死亡风险增加与较高的NPAR相关。NPAR被认为是90天全因死亡率的良好预测指标。在温州医科大学附属第二医院,较高的NPAR与30天和90天死亡率风险较高相关。