Department of Diagnostic and Interventional Radiology, University Hospital Bonn, Venusberg-Campus 1, 53127, Bonn, Germany.
Quantitative Imaging Lab Bonn (QILaB), Venusberg-Campus 1, 53127, Bonn, Germany.
BMC Neurol. 2023 Feb 28;23(1):86. doi: 10.1186/s12883-023-03132-7.
Outcome assessment in stroke patients is essential for evidence-based stroke care planning. Computed tomography (CT) is the mainstay of diagnosis in acute stroke. This study aimed to investigate whether CT-derived cervical fat-free muscle fraction (FFMF) as a biomarker of muscle quality is associated with outcome parameters after acute ischemic stroke.
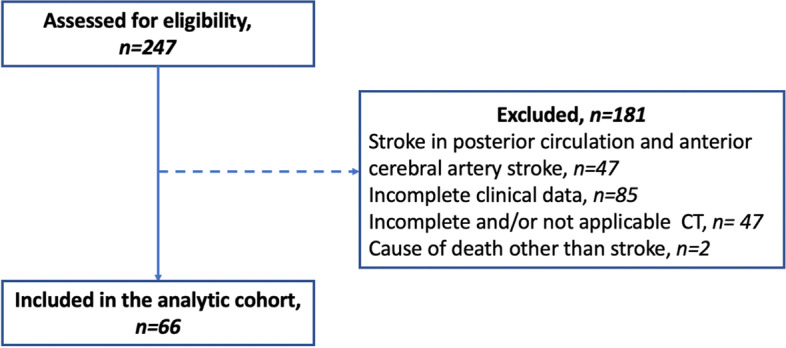
In this retrospective study, 66 patients (mean age: 76 ± 13 years, 30 female) with acute ischemic stroke in the anterior circulation who underwent CT, including CT-angiography, and endovascular mechanical thrombectomy of the middle cerebral artery between August 2016 and January 2020 were identified. Based on densitometric thresholds, cervical paraspinal muscles covered on CT-angiography were separated into areas of fatty and lean muscle and FFMF was calculated. The study cohort was binarized based on median FFMF (cutoff value: < 71.6%) to compare clinical variables and outcome data between two groups. Unpaired t test and Mann-Whitney U test were used for statistical analysis.
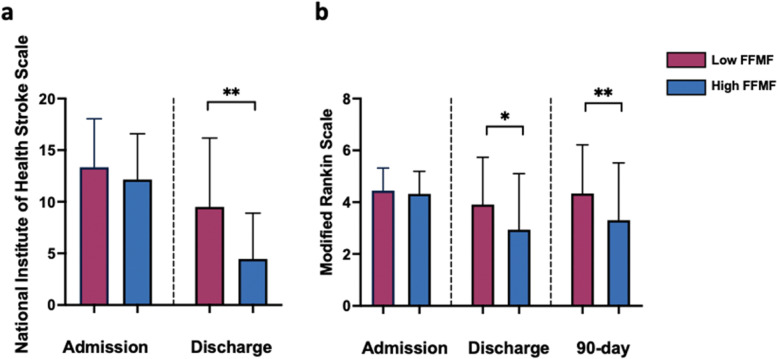
National Institute of Health Stroke Scale (NIHSS) (12.2 ± 4.4 vs. 13.6 ± 4.5, P = 0.297) and modified Rankin scale (mRS) (4.3 ± 0.9 vs. 4.4 ± 0.9, P = 0.475) at admission, and pre-stroke mRS (1 ± 1.3 vs. 0.9 ± 1.4, P = 0.489) were similar between groups with high and low FFMF. NIHSS and mRS at discharge were significantly better in patients with high FFMF compared to patients with low FFMF (NIHSS: 4.5 ± 4.4 vs. 9.5 ± 6.7; P = 0.004 and mRS: 2.9 ± 2.1 vs.3.9 ± 1.8; P = 0.049). 90-day mRS was significantly better in patients with high FFMF compared to patients with low FFMF (3.3 ± 2.2 vs. 4.3 ± 1.9, P = 0.045).
Cervical FFMF obtained from routine clinical CT might be a new imaging-based muscle quality biomarker for outcome prediction in stroke patients.
对脑卒中患者进行结局评估对于基于证据的脑卒中护理计划至关重要。计算机断层扫描(CT)是急性脑卒中诊断的主要手段。本研究旨在探讨 CT 衍生的颈段去脂肌肉分数(FFMF)作为肌肉质量的生物标志物是否与急性缺血性脑卒中后的结局参数相关。
在这项回顾性研究中,共纳入了 2016 年 8 月至 2020 年 1 月期间接受 CT(包括 CT 血管造影和大脑中动脉血管内机械血栓切除术)检查的 66 例前循环急性缺血性脑卒中患者(平均年龄:76±13 岁,30 例女性)。基于密度测定阈值,将 CT 血管造影上覆盖的颈段椎旁肌肉分为脂肪和肌肉区域,并计算 FFMF。根据中位数 FFMF(截断值:<71.6%)将研究队列分为两组,比较两组间的临床变量和结局数据。采用配对 t 检验和 Mann-Whitney U 检验进行统计学分析。
入院时 NIHSS(12.2±4.4 vs. 13.6±4.5,P=0.297)和改良 Rankin 量表(mRS)(4.3±0.9 vs. 4.4±0.9,P=0.475)以及预发病 mRS(1±1.3 vs. 0.9±1.4,P=0.489)在 FFMF 高组和低组间相似。与 FFMF 低组相比,FFMF 高组患者出院时 NIHSS 和 mRS 明显更好(NIHSS:4.5±4.4 vs. 9.5±6.7;P=0.004,mRS:2.9±2.1 vs. 3.9±1.8;P=0.049)。90 天 mRS 评分在 FFMF 高组明显优于 FFMF 低组(3.3±2.2 vs. 4.3±1.9,P=0.045)。
从常规临床 CT 获得的颈段 FFMF 可能是一种新的基于影像学的脑卒中患者结局预测的肌肉质量生物标志物。