Department of Psychology, University of Pennsylvania, Philadelphia, PA, USA.
J Child Psychol Psychiatry. 2023 Sep;64(9):1372-1387. doi: 10.1111/jcpp.13774. Epub 2023 Mar 1.
Children with callous-unemotional (CU) traits are at high lifetime risk of antisocial behavior. It is unknown if treatments for disruptive behavior disorders are as effective for children with CU traits (DBD+CU) as those without (DBD-only), nor if treatments directly reduce CU traits. Separate multilevel meta-analyses were conducted to compare treatment effects on DBD symptoms for DBD+CU versus DBD-only children and evaluate direct treatment-related reductions in CU traits, as well as to examine moderating factors for both questions.
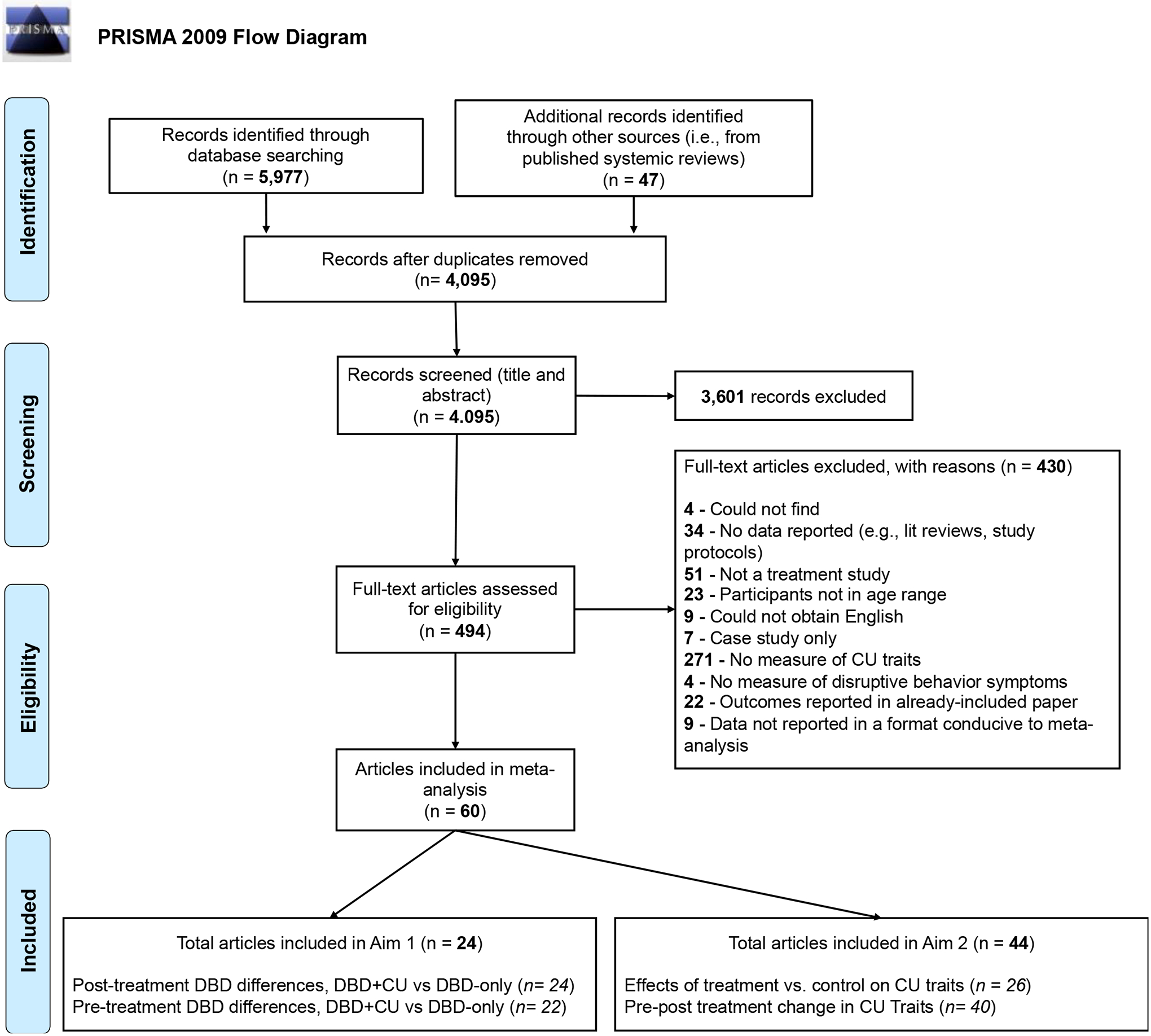
We systematically searched PsycINFO, PubMed, Cochran Library (Trials), EMBASE, MEDLINE, APA PsycNet, Scopus, and Web of Science. Eligible studies were randomized controlled trials, controlled trials, and uncontrolled studies evaluating child-focused, parenting-focused, pharmacological, family-focused, or multimodal treatments.
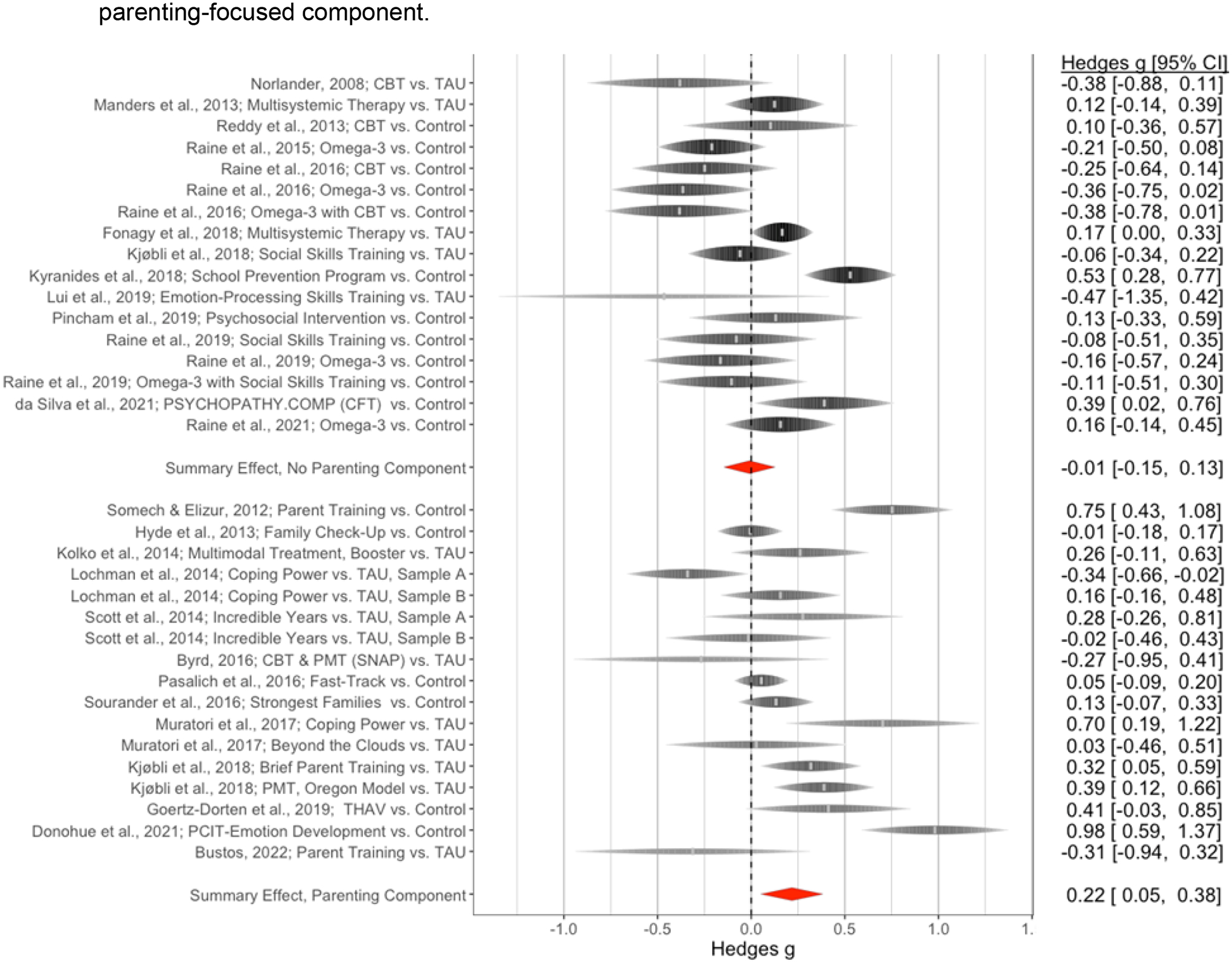
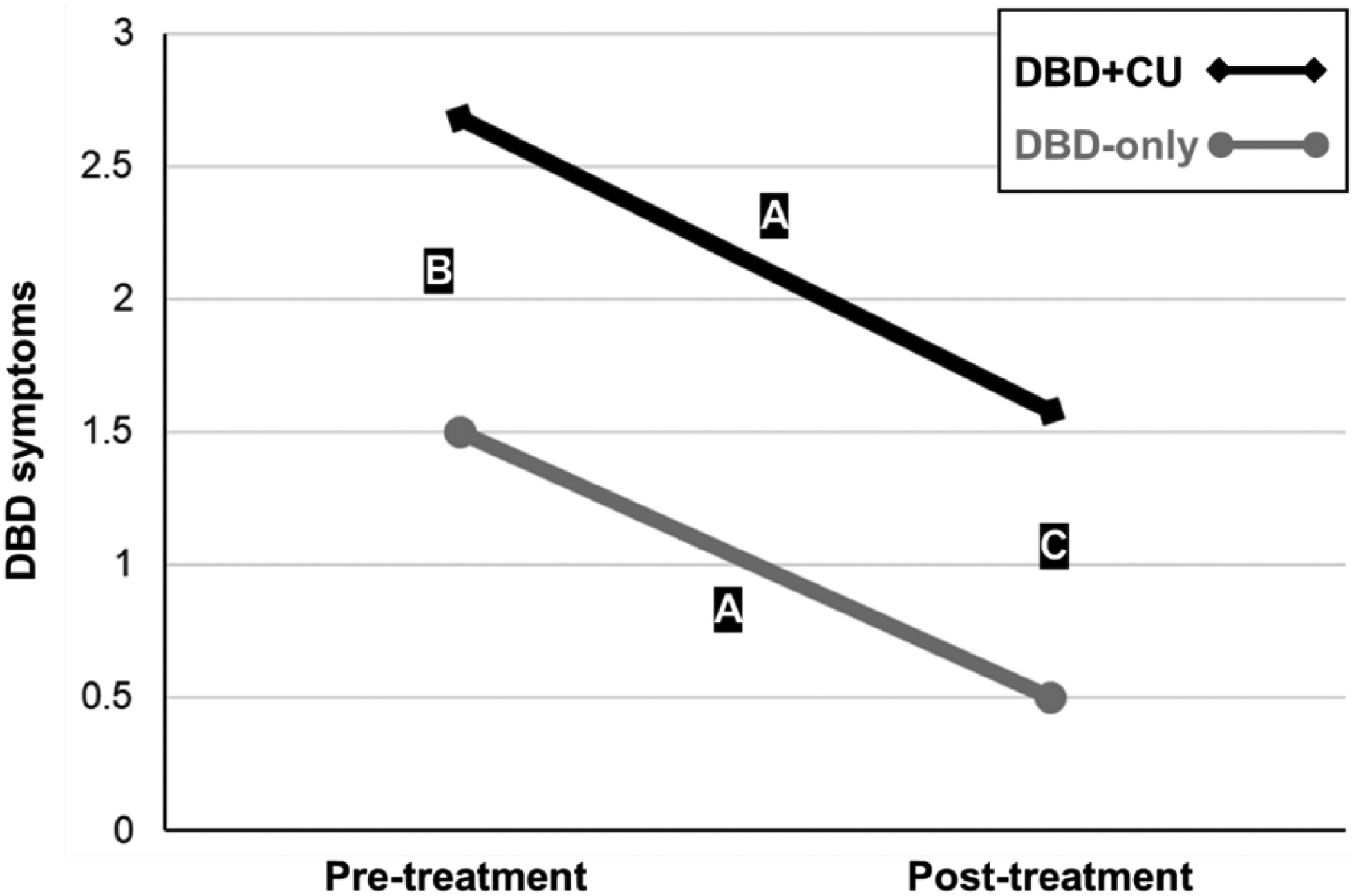
Sixty studies with 9,405 participants were included (M = 10.04, SD = 3.89 years, 25.09% female, 44.10% racial/ethnic minority). First, treatment was associated with similar reductions in DBD symptoms for DBD+CU (SMD = 1.08, 95% CI = 0.45, 1.72) and DBD-only (SMD = 1.01, 95% CI = 0.38, 1.64). However, DBD+CU started (SMD = 1.18, 95% CI = 0.57, 1.80) and ended (SMD = 0.73, p < .001; 95% CI = 0.43, 1.04) treatment with more DBD symptoms. Second, although there was no overall direct effect of treatment on CU traits (SMD = .09, 95% CI = -0.02, 0.20), there were moderating factors. Significant treatment-related reductions in CU traits were found for studies testing parenting-focused components (SMD = 0.21, 95% CI = 0.06, 0.35), using parent-reported measures (SMD = 0.16, 95% CI = 0.04, 0.28), rated as higher quality (SMD = 0.26, 95% CI = 0.13, 0.39), conducted outside the United States (SMD = 0.19, 95% CI = 0.05, 0.32), and with less than half the sample from a racial/ethnic minority group (SMD = 0.15, 95% CI = 0.002, 0.30).
DBD+CU children improve with treatment, but their greater DBD symptom severity requires specialized treatment modules that could be implemented alongside parenting programs. Conclusions are tempered by heterogeneity across studies and scant evidence from randomized controlled trials.
具有无情无情感(CU)特征的儿童终生患有反社会行为的风险很高。目前尚不清楚针对破坏性行为障碍(DBD)的治疗方法对具有 CU 特征的儿童(DBD+CU)是否与不具有 CU 特征的儿童(DBD-only)一样有效,也不知道治疗方法是否直接减少 CU 特征。分别进行了多层次荟萃分析,以比较 DBD+CU 与 DBD-only 儿童的治疗对 DBD 症状的影响,并评估治疗对 CU 特征的直接相关减少,以及检查这两个问题的调节因素。
我们系统地搜索了 PsycINFO、PubMed、Cochran 图书馆(试验)、EMBASE、MEDLINE、APA PsycNet、Scopus 和 Web of Science。合格的研究是随机对照试验、对照试验和非对照研究,评估以儿童为中心、以父母为中心、药物治疗、以家庭为中心或多模式治疗。
共有 60 项研究纳入了 9405 名参与者(M = 10.04,SD = 3.89 岁,25.09%为女性,44.10%为少数族裔)。首先,治疗与 DBD+CU(SMD = 1.08,95%CI = 0.45,1.72)和 DBD-only(SMD = 1.01,95%CI = 0.38,1.64)的 DBD 症状改善相关。然而,DBD+CU 开始(SMD = 1.18,95%CI = 0.57,1.80)和结束(SMD = 0.73,p < 0.001;95%CI = 0.43,1.04)治疗时的 DBD 症状更多。其次,尽管治疗对 CU 特征没有总体直接影响(SMD = 0.09,95%CI = -0.02,0.20),但存在调节因素。对于测试以父母为中心的组成部分的研究(SMD = 0.21,95%CI = 0.06,0.35),使用父母报告的测量方法(SMD = 0.16,95%CI = 0.04,0.28),评分较高的研究(SMD = 0.26,95%CI = 0.13,0.39),在美国境外进行的研究(SMD = 0.19,95%CI = 0.05,0.32),以及样本中不到一半来自少数族裔群体的研究(SMD = 0.15,95%CI = 0.002,0.30),发现治疗与 CU 特征的显著相关减少。
DBD+CU 儿童通过治疗得到改善,但他们更严重的 DBD 症状需要专门的治疗模块,可以与父母计划一起实施。研究的异质性和随机对照试验的证据稀少限制了结论的推广。