Taghavi Katayoun, Mandiriri Ardele, Shamu Tinei, Rohner Eliane, Bütikofer Lukas, Asangbeh Serra, Magure Tsitsi, Chimbetete Cleophas, Egger Matthias, Pascoe Margaret, Bohlius Julia
Institute of Social and Preventive Medicine, University of Bern, Bern, Switzerland.
The Graduate School for Cellular and Biomedical Sciences of the University of Bern, Bern, Switzerland.
PLOS Glob Public Health. 2022;2(2). doi: 10.1371/journal.pgph.0000156. Epub 2022 Feb 2.
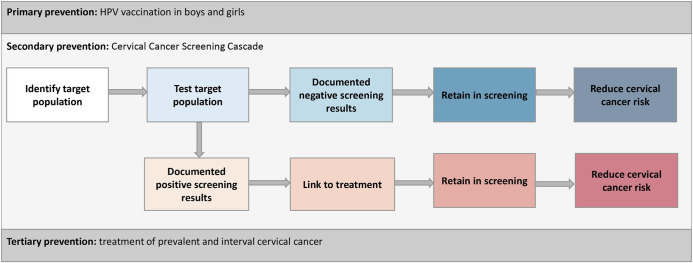
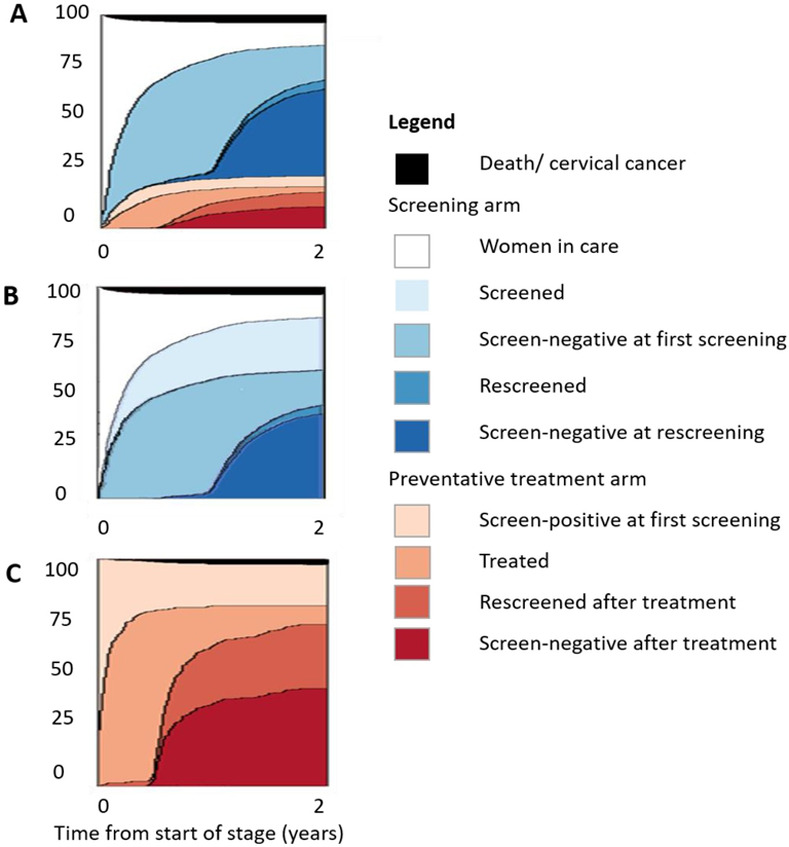
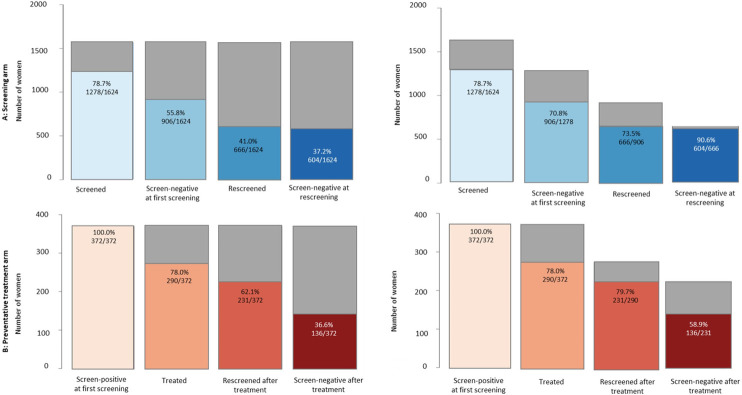
Countries with high HIV prevalence, predominantly in sub-Sahahran Africa, have the highest cervical cancer rates globally. HIV care cascades successfully facilitated the scale-up of antiretroviral therapy. A cascade approach could similarly succeed to scale-up cervical cancer screening, supporting WHO's goal to eliminate cervical cancer. We defined a Cervical Cancer Screening Cascade for women living with HIV (WLHIV), evaluating the continuum of cervical cancer screening integrated into an HIV clinic in Zimbabwe. We included WLHIV aged ≥18 years enrolled at Newlands Clinic in Harare from June 2012-2017 and followed them until June 2018. We used a cascade approach to evaluate the full continuum of secondary prevention from screening to treatment of pre-cancer and follow-up. We report percentages, median time to reach cascade stages, and cumulative incidence at two years with 95% confidence intervals (CI). We used univariable Cox proportional hazard regressions to calculate cause-specific hazard ratios with 95% CIs for factors associated with completing the cascade stages. We included 1624 WLHIV in the study. The cumulative incidence of cervical screening was 85.4% (95% CI 83.5-87.1) at two years. Among the 396 WLHIV who received screen-positive tests in the study, the cumulative incidence of treatment after a positive screening test was 79.5% (95% CI 75.1-83.2) at two years. The cumulative incidence of testing negative at re-screening after treatment was 36.1% (95% CI 31.2-40.7) at two years. Using a cascade approach to evaluate the full continuum of cervical cancer screening, we found less-than 80% of WLHIV received treatment after screen-positive tests and less-than 40% were screen-negative at follow-up. Interventions to improve linkage to treatment for screen-positive WLHIV and studies to understand the clinical significance of screen-positive tests at follow-up among WLHIV are needed. These gaps in the continuum of care must be addressed in order to prevent cervical cancer.
艾滋病毒感染率较高的国家主要分布在撒哈拉以南非洲,这些国家的宫颈癌发病率是全球最高的。艾滋病毒治疗连续护理成功推动了抗逆转录病毒疗法的扩大应用。类似地,一种连续护理方法可能会成功扩大宫颈癌筛查规模,支持世界卫生组织消除宫颈癌的目标。我们为感染艾滋病毒的女性(WLHIV)定义了一种宫颈癌筛查连续护理模式,评估了津巴布韦一家艾滋病毒诊所整合的宫颈癌筛查连续过程。我们纳入了2012年6月至2017年在哈拉雷纽兰兹诊所登记的年龄≥18岁的感染艾滋病毒女性,并对她们进行随访直至2018年6月。我们采用连续护理方法来评估从筛查到癌前病变治疗及随访的二级预防全过程。我们报告了百分比、达到连续护理阶段的中位时间以及两年时的累积发病率,并给出95%置信区间(CI)。我们使用单变量Cox比例风险回归来计算与完成连续护理阶段相关因素的特定病因风险比及95%置信区间。我们的研究纳入了1624名感染艾滋病毒女性。两年时宫颈癌筛查的累积发病率为85.4%(95%CI 83.5 - 87.1)。在研究中接受筛查结果为阳性的396名感染艾滋病毒女性中,筛查结果为阳性后两年时治疗的累积发病率为79.5%(95%CI 75.1 - 83.2)。治疗后再次筛查结果为阴性的两年累积发病率为36.1%(95%CI 31.2 - 40.7)。通过采用连续护理方法评估宫颈癌筛查的全过程,我们发现筛查结果为阳性的感染艾滋病毒女性中不到80%接受了治疗,随访时不到40%的筛查结果为阴性。需要采取干预措施来改善筛查结果为阳性的感染艾滋病毒女性与治疗的衔接,并开展研究以了解感染艾滋病毒女性随访时筛查结果为阳性的临床意义。必须解决护理连续过程中的这些差距,以预防宫颈癌。