Department of Cancer Immunology, Institute for Cancer Research, Oslo University Hospital, Oslo, Norway; KG Jebsen Centre for B cell malignancies, Institute of Clinical Medicine, Faculty of Medicine, University of Oslo, Oslo.
Department of Oncology and Medical Physics, Haukeland University Hospital, Bergen.
Haematologica. 2023 Sep 1;108(9):2454-2466. doi: 10.3324/haematol.2022.282289.
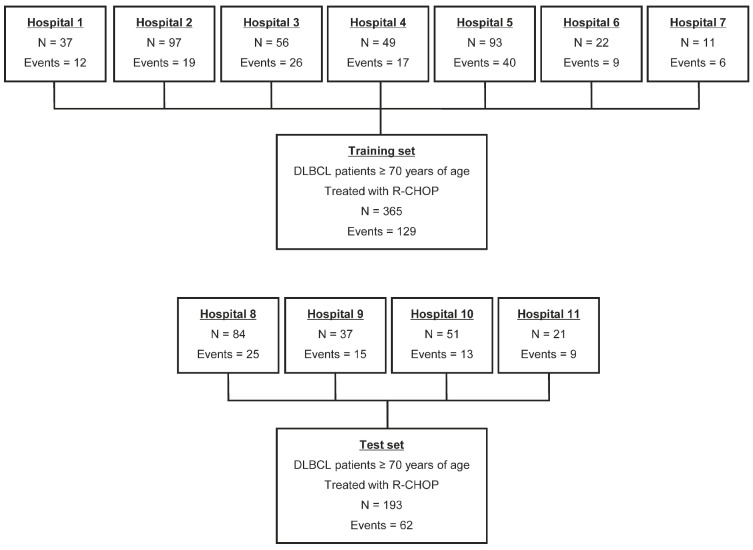
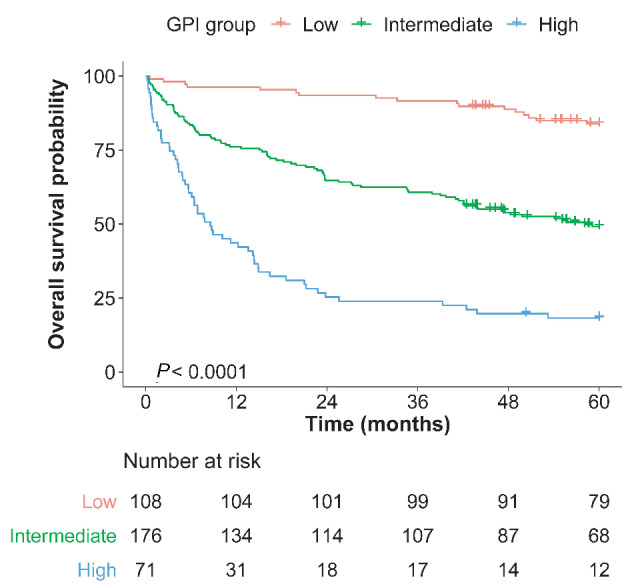
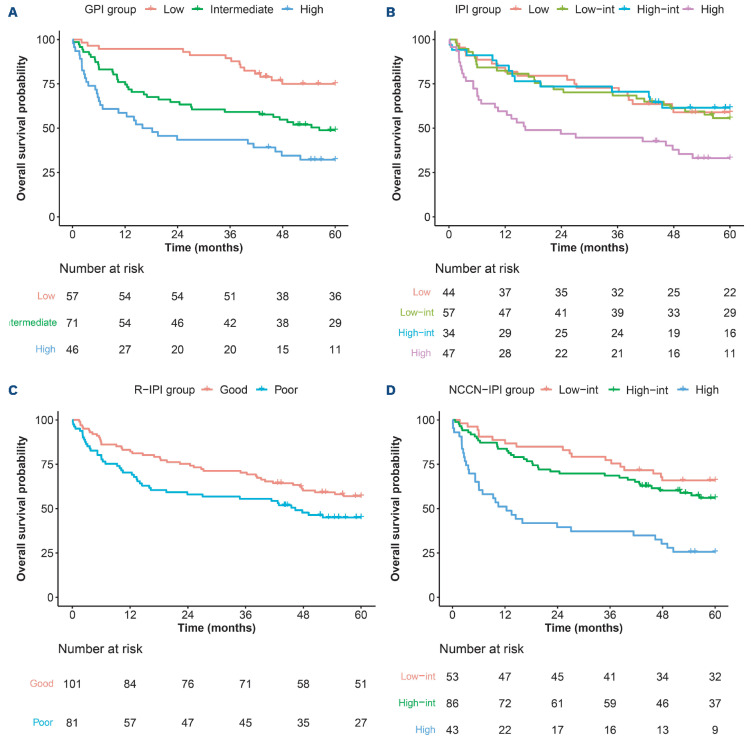
The International prognostic Index (IPI) is the most widely used clinical prediction model for diffuse large B-cell lymphoma (DLBCL) patients treated with rituximab, cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP), but may be suboptimal in older patients. We aimed to develop and externally validate a clinical prediction model for older, RCHOP- treated DLBCL patients by examining geriatric assessment and lymphoma-related parameters in real-world cohorts. A population-based training set of 365 R-CHOP-treated DLBCL patients ≥70 years was identified through the Cancer Registry of Norway. The external test set consisted of a population-based cohort of 193 patients. Data on candidate predictors were retrieved from the Cancer Registry and through review of clinical records. Cox regression models for 2-year overall survival were used for model selection. Activities of daily living, the Charlson Comorbidity Index, age, sex, albumin, stage, Eastern Cooperative Oncology Group performance status and lactate dehydrogenase level were identified as independent predictors and combined into a Geriatric Prognostic Index (GPI). The GPI demonstrated good discrimination (optimismcorrected C-index 0.752), and identified low-, intermediate- and high-risk groups with significantly different survivals (2- year overall survival, 94%, 65%, and 25%, respectively). At external validation, the continuous and grouped GPI demonstrated good discrimination (C-index 0.727 and 0.710, respectively) and the GPI groups had significantly different survivals (2-year overall survival 95%, 65%, and 44%, respectively). Both the continuous and grouped GPI showed better discrimination than the IPI, revised-IPI and National Comprehensive Cancer Network (NCCN)-IPI (C-index 0.621, 0.583, and 0.670, respectively). In conclusion, we have developed and externally validated a GPI for older DLBCL patients treated with R-CHOP that outperformed the IPI, revised-IPI and NCCN-IPI. A web-based calculator is available at https://wide.shinyapps. io/GPIcalculator/.
国际预后指数(IPI)是接受利妥昔单抗、环磷酰胺、多柔比星、长春新碱和泼尼松(R-CHOP)治疗弥漫性大 B 细胞淋巴瘤(DLBCL)患者最广泛使用的临床预测模型,但在老年患者中可能并不理想。我们旨在通过检查真实世界队列中的老年 R-CHOP 治疗 DLBCL 患者的老年评估和淋巴瘤相关参数,开发和外部验证一种用于老年 R-CHOP 治疗 DLBCL 患者的临床预测模型。通过挪威癌症登记处确定了一个包含 365 名接受 R-CHOP 治疗且年龄≥70 岁的 DLBCL 患者的基于人群的训练集。外部测试集由 193 名基于人群的患者组成。从癌症登记处和临床记录回顾中检索候选预测因子的数据。用于 2 年总生存的 Cox 回归模型用于模型选择。日常生活活动、Charlson 合并症指数、年龄、性别、白蛋白、分期、东部合作肿瘤组表现状态和乳酸脱氢酶水平被确定为独立预测因子,并组合成老年预后指数(GPI)。GPI 表现出良好的区分度(校正后的 optimism-corrected C 指数为 0.752),并确定了具有显著不同生存的低、中、高危组(2 年总生存率分别为 94%、65%和 25%)。在外部验证中,连续和分组 GPI 表现出良好的区分度(C 指数分别为 0.727 和 0.710),并且 GPI 组具有显著不同的生存率(2 年总生存率分别为 95%、65%和 44%)。连续和分组 GPI 的区分度均优于 IPI、修订 IPI 和国家综合癌症网络(NCCN)-IPI(C 指数分别为 0.621、0.583 和 0.670)。总之,我们已经开发并验证了一种用于接受 R-CHOP 治疗的老年 DLBCL 患者的 GPI,其性能优于 IPI、修订 IPI 和 NCCN-IPI。一个基于网络的计算器可在 https://wide.shinyapps.io/GPIcalculator/ 上获得。