Department of Gastroenterology, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan.
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Nihon University School of Medicine, Tokyo, Japan.
Support Care Cancer. 2023 Mar 2;31(3):197. doi: 10.1007/s00520-023-07659-w.
Patients with pancreatic cancer often have cancer cachexia at diagnosis. Recent studies suggested that loss of skeletal muscle mass was related to cancer cachexia, which hindered continuance of chemotherapy and could be one of prognostic factors in pancreatic cancer, however the association remains unclear in patients receiving gemcitabine and nab-paclitaxel (GnP).
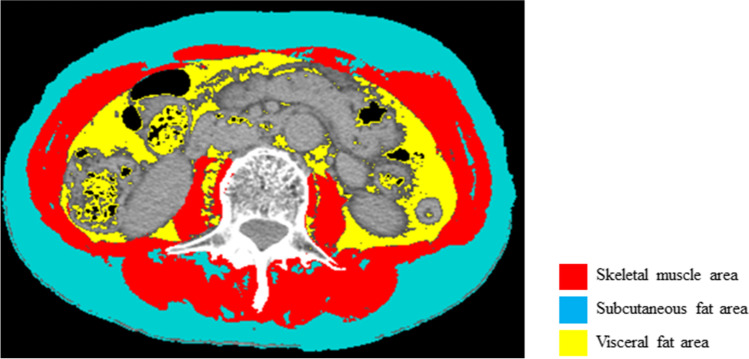
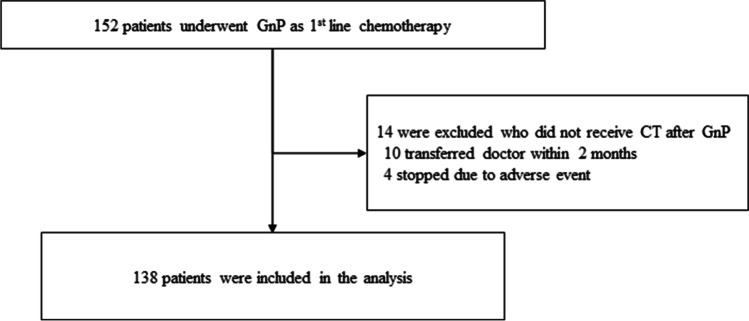
We retrospectively studied 138 patients with unresectable pancreatic cancer receiving first-line GnP at the University of Tokyo from January 2015 to September 2020. We calculated body composition in CT images before chemotherapy and at initial evaluation, and evaluated the association of both body composition before chemotherapy and its changes at initial evaluation.
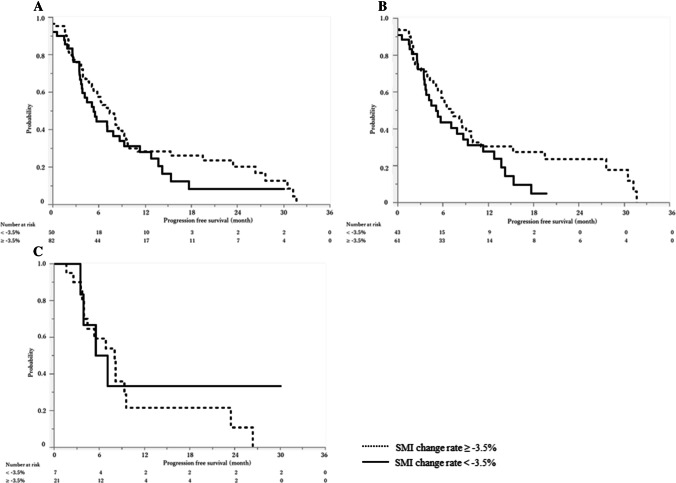
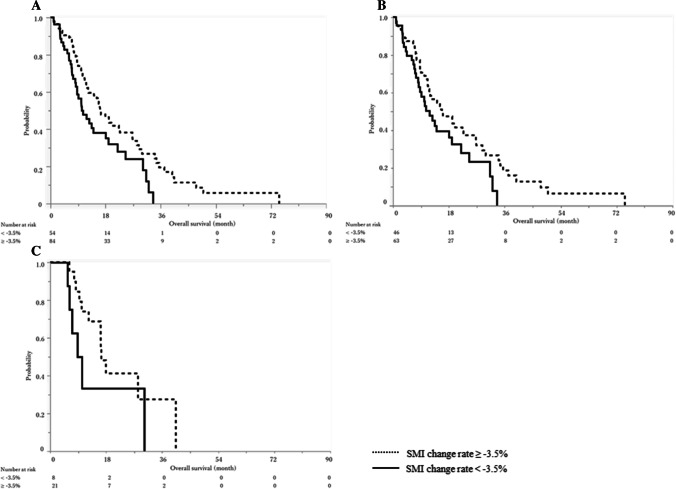
Compared by skeletal muscle mass index (SMI) change rate between pre-chemotherapy and initial evaluation, there were statistically significantly differences in the median OS: 16.3 months (95%CI 12.3-22.7) and 10.3 months (95%CI 8.3-18.1) between SMI change rate ≥ -3.5% and < -3.5% groups (P = 0.01). By multivariate analysis for OS, CA19-9 (HR 3.34, 95%CI 2.00-5.57, P < 0.01), PLR (HR 1.68, 95%CI 1.01-2.78, P = 0.04), mGPS (HR 2.32, 95%CI 1.47-3.65, P < 0.01) and relative dose intensity (HR 2.21, 95%CI 1.42-3.46, P < 0.01) were significantly poor prognostic factors. SMI change rate (HR 1.47, 95%CI 0.95-2.28, P = 0.08) showed a trend to poor prognosis. Sarcopenia before chemotherapy was not significantly associated with PFS or OS.
Early skeletal muscle mass decline was associated with poor OS. Further investigation is warranted whether the maintenance of skeletal muscle mass by nutritional support would improve prognosis.
胰腺癌患者在诊断时常伴有癌性恶病质。最近的研究表明,骨骼肌量的丢失与癌性恶病质有关,这阻碍了化疗的继续进行,并且可能是胰腺癌的预后因素之一,然而在接受吉西他滨和 nab-紫杉醇(GnP)治疗的患者中,这种关联尚不清楚。
我们回顾性研究了 2015 年 1 月至 2020 年 9 月在东京大学接受一线 GnP 治疗的 138 例不可切除的胰腺癌患者。我们在化疗前和初始评估时计算 CT 图像中的身体成分,并评估化疗前的身体成分及其在初始评估时的变化之间的相关性。
根据化疗前和初始评估时骨骼肌质量指数(SMI)变化率的比较,SMI 变化率≥-3.5%和< -3.5%组之间的中位 OS 存在统计学显著差异:16.3 个月(95%CI 12.3-22.7)和 10.3 个月(95%CI 8.3-18.1)(P=0.01)。对于 OS 的多变量分析,CA19-9(HR 3.34,95%CI 2.00-5.57,P<0.01)、PLR(HR 1.68,95%CI 1.01-2.78,P=0.04)、mGPS(HR 2.32,95%CI 1.47-3.65,P<0.01)和相对剂量强度(HR 2.21,95%CI 1.42-3.46,P<0.01)是显著的不良预后因素。SMI 变化率(HR 1.47,95%CI 0.95-2.28,P=0.08)也显示出不良预后的趋势。化疗前的肌肉减少症与 PFS 或 OS 无显著相关性。
早期骨骼肌质量下降与 OS 不良相关。是否通过营养支持维持骨骼肌质量会改善预后,还需要进一步研究。