Division of Cardiothoracic Anesthesiology, Department of Anesthesiology and Perioperative Medicine, University of California, Los Angeles, CA.
Division of Cardiac Surgery, Department of Surgery, University of California, Los Angeles, CA.
J Cardiothorac Vasc Anesth. 2023 May;37(5):732-747. doi: 10.1053/j.jvca.2023.01.006. Epub 2023 Jan 9.
The primary objective of this study was to evaluate whether the COVID-19 pandemic altered the racial and ethnic composition of patients receiving cardiac procedural care.
This was a retrospective observational study.
This study was conducted at a single tertiary-care university hospital.
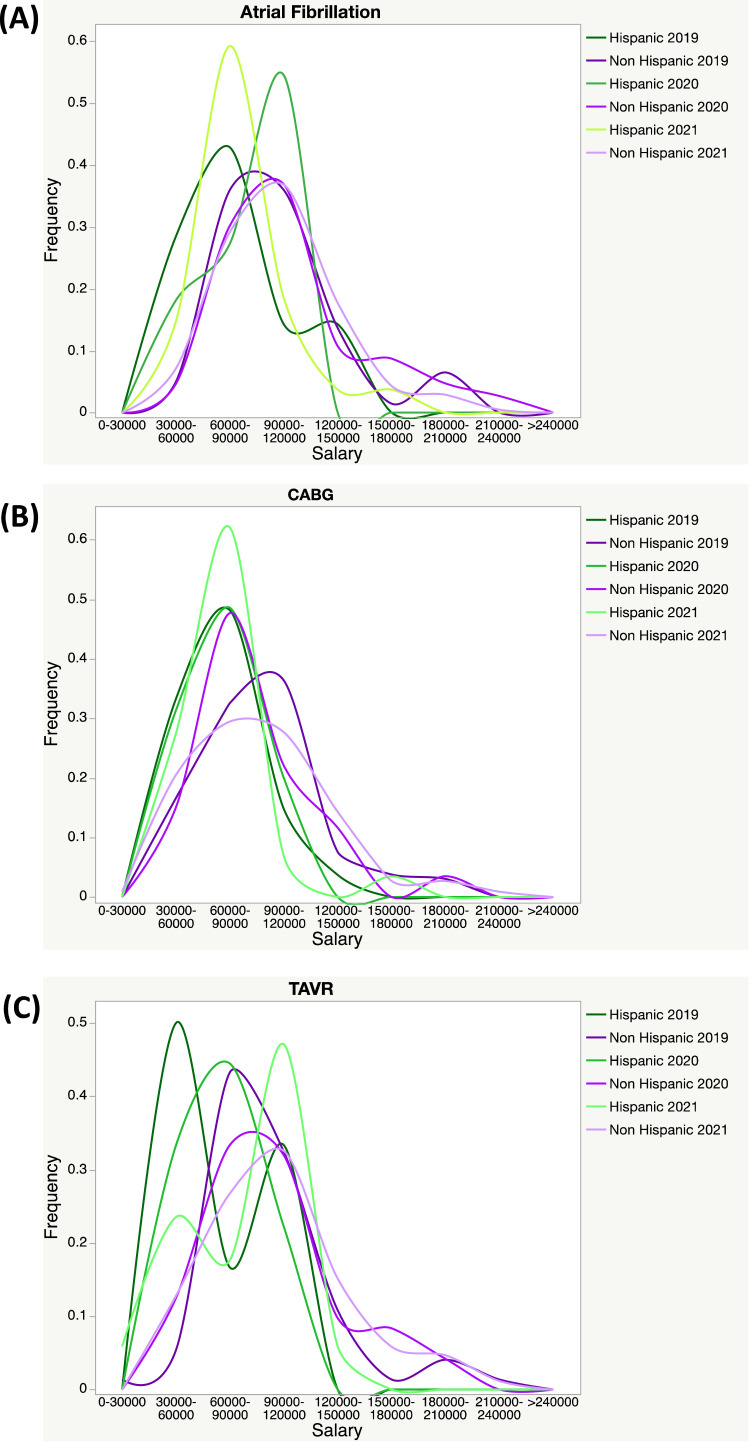
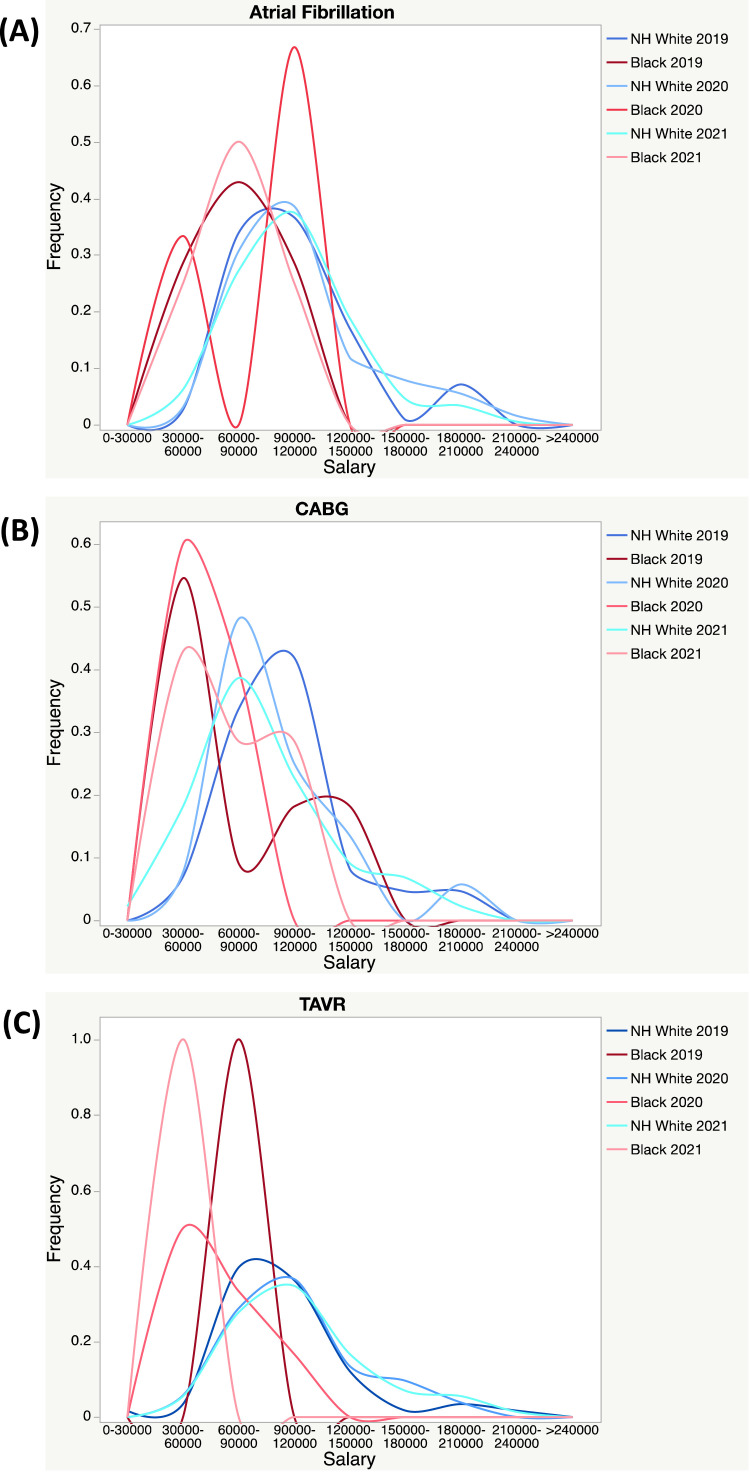
A total of 1,704 adult patients undergoing transcatheter aortic valve replacement (TAVR) (n = 413), coronary artery bypass grafting (CABG) (n = 506), or atrial fibrillation (AF) ablation (n = 785) from March 2019 through March 2022 were included in this study.
No interventions were performed as this was a retrospective observational study.
Patients were grouped based on the date of their procedure: pre-COVID (March 2019 to February 2020), COVID Year 1 (March 2020 to February 2021), and COVID Year 2 (March 2021 to March 2022). Population-adjusted procedural incidence rates during each period were examined and stratified based on race and ethnicity. The procedural incidence rate was higher for White patients versus Black, and non-Hispanic patients versus Hispanic patients for every procedure and every period. For TAVR, the difference in procedural rates between White patients versus Black patients decreased between the pre-COVID and COVID Year 1 (12.05-6.34 per 1,000,000 persons). For CABG, the difference in procedural rates between White patients versus Black, and non-Hispanic patients versus Hispanic patients did not change significantly. For AF ablations, the difference in procedural rates between White patients versus Black patients increased over time (13.06 to 21.55 to 29.64 per 1,000,000 persons in the pre-COVID, COVID Year 1, and COVID Year 2, respectively).
Racial and ethnic disparities in access to cardiac procedural care were present throughout all study time periods at the authors' institution. Their findings reinforce the continuing need for initiatives to reduce racial and ethnic disparities in healthcare. Further studies are needed to fully elucidate the effects of the COVID-19 pandemic on healthcare access and delivery.
本研究的主要目的是评估 COVID-19 大流行是否改变了接受心脏介入治疗的患者的种族和民族构成。
这是一项回顾性观察性研究。
本研究在一家单中心三级保健大学医院进行。
本研究共纳入了 2019 年 3 月至 2022 年 3 月期间接受经导管主动脉瓣置换术(TAVR)(n=413)、冠状动脉旁路移植术(CABG)(n=506)或心房颤动(AF)消融术(n=785)的 1704 名成年患者。
由于这是一项回顾性观察性研究,因此未进行任何干预。
根据手术日期将患者分为三组:COVID-19 前(2019 年 3 月至 2020 年 2 月)、COVID-19 第 1 年(2020 年 3 月至 2021 年 2 月)和 COVID-19 第 2 年(2021 年 3 月至 2022 年 3 月)。检查了每个时期的人群调整后程序发生率,并根据种族和民族进行分层。对于每一种手术和每一个时期,白人患者的手术发生率均高于黑人患者和非西班牙裔患者。对于 TAVR,COVID-19 前和 COVID-1 年间白人与黑人患者之间的手术率差异有所缩小(每 100 万人中 12.05-6.34 例)。对于 CABG,白人与黑人患者以及非西班牙裔患者与西班牙裔患者之间的手术率差异无显著变化。对于 AF 消融术,白人与黑人患者之间的手术率差异随着时间的推移而增加(COVID-19 前、COVID-1 年和 COVID-1 年分别为每 100 万人中 13.06、21.55 和 29.64 例)。
在研究期间,作者所在机构所有研究时间段均存在心脏介入治疗机会方面的种族和民族差异。他们的发现强调了继续采取举措减少医疗保健领域种族和民族差异的必要性。需要进一步研究以充分阐明 COVID-19 大流行对医疗保健获取和提供的影响。