Faculty of Medicine, The University of Queensland, Brisbane, Australia.
Swedish University of Agricultural Sciences, Uppsala, Sweden.
BMC Pregnancy Childbirth. 2023 Mar 2;23(1):137. doi: 10.1186/s12884-022-05221-w.
The reproductive hormone oxytocin facilitates labour, birth and postpartum adaptations for women and newborns. Synthetic oxytocin is commonly given to induce or augment labour and to decrease postpartum bleeding.
To systematically review studies measuring plasma oxytocin levels in women and newborns following maternal administration of synthetic oxytocin during labour, birth and/or postpartum and to consider possible impacts on endogenous oxytocin and related systems.
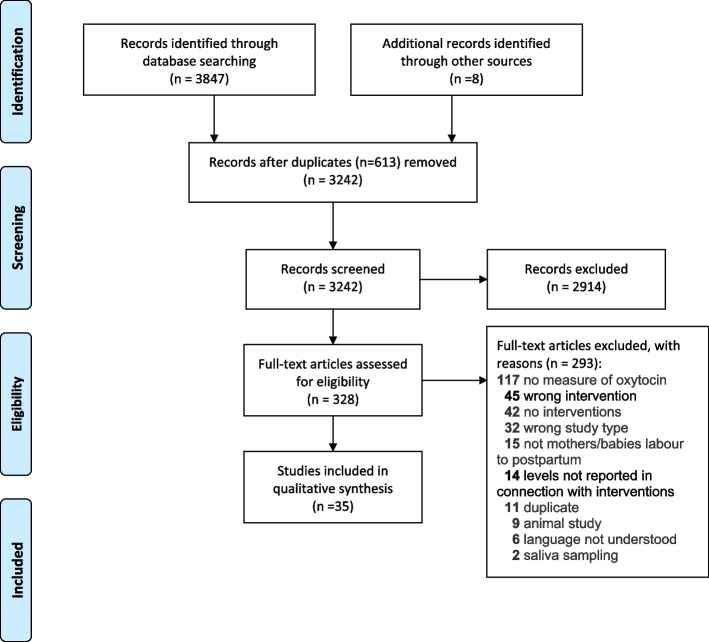
Systematic searches of PubMed, CINAHL, PsycInfo and Scopus databases followed PRISMA guidelines, including all peer-reviewed studies in languages understood by the authors. Thirty-five publications met inclusion criteria, including 1373 women and 148 newborns. Studies varied substantially in design and methodology, so classical meta-analysis was not possible. Therefore, results were categorized, analysed and summarised in text and tables.
Infusions of synthetic oxytocin increased maternal plasma oxytocin levels dose-dependently; doubling the infusion rate approximately doubled oxytocin levels. Infusions below 10 milliunits per minute (mU/min) did not raise maternal oxytocin above the range observed in physiological labour. At high intrapartum infusion rates (up to 32 mU/min) maternal plasma oxytocin reached 2-3 times physiological levels. Postpartum synthetic oxytocin regimens used comparatively higher doses with shorter duration compared to labour, giving greater but transient maternal oxytocin elevations. Total postpartum dose was comparable to total intrapartum dose following vaginal birth, but post-caesarean dosages were higher. Newborn oxytocin levels were higher in the umbilical artery vs. umbilical vein, and both were higher than maternal plasma levels, implying substantial fetal oxytocin production in labour. Newborn oxytocin levels were not further elevated following maternal intrapartum synthetic oxytocin, suggesting that synthetic oxytocin at clinical doses does not cross from mother to fetus.
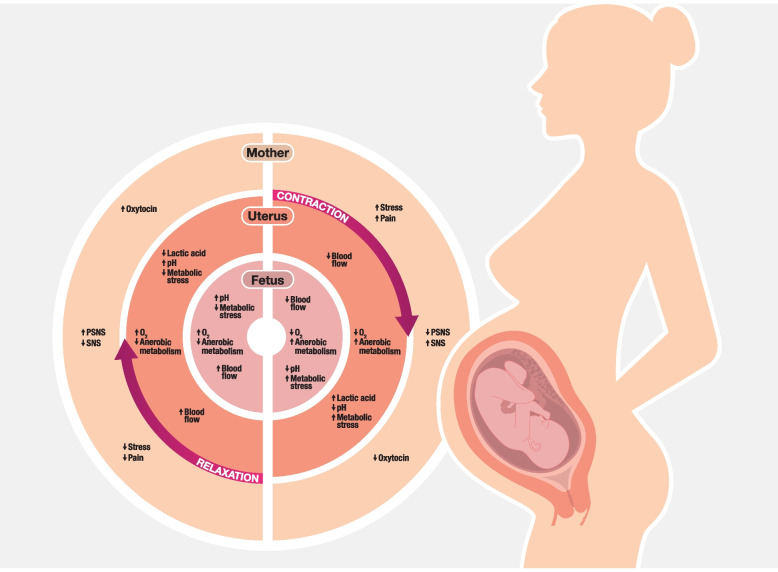
Synthetic oxytocin infusion during labour increased maternal plasma oxytocin levels 2-3-fold at the highest doses and was not associated with neonatal plasma oxytocin elevations. Therefore, direct effects from synthetic oxytocin transfer to maternal brain or fetus are unlikely. However, infusions of synthetic oxytocin in labour change uterine contraction patterns. This may influence uterine blood flow and maternal autonomic nervous system activity, potentially harming the fetus and increasing maternal pain and stress.
生殖激素催产素有助于女性和新生儿分娩、出生和产后适应。合成催产素常用于诱导或增强分娩和减少产后出血。
系统综述研究测量产妇分娩、出生和/或产后给予合成催产素后女性和新生儿的血浆催产素水平,并考虑对内源性催产素和相关系统的可能影响。
根据 PRISMA 指南,对 PubMed、CINAHL、PsycInfo 和 Scopus 数据库进行系统搜索,包括作者理解的所有同行评议研究。符合纳入标准的 35 篇文献包括 1373 名女性和 148 名新生儿。这些研究在设计和方法上差异很大,因此无法进行经典的荟萃分析。因此,结果以文字和表格的形式进行分类、分析和总结。
合成催产素输注剂量依赖性地增加产妇血浆催产素水平;输注率增加一倍,催产素水平增加一倍左右。每分钟输注量低于 10 毫单位(mU/min)不会使产妇的催产素水平升高到生理分娩时观察到的范围之上。在分娩时高的输注率(高达 32 mU/min)下,产妇血浆催产素达到生理水平的 2-3 倍。与分娩相比,产后合成催产素方案使用的剂量较高,持续时间较短,使产妇的催产素水平短暂升高。总产后剂量与阴道分娩后的总分娩剂量相当,但剖宫产后的剂量较高。脐动脉中的新生儿催产素水平高于脐静脉,两者均高于产妇的血浆水平,这意味着在分娩过程中胎儿大量产生催产素。新生儿催产素水平在产妇分娩时接受合成催产素后没有进一步升高,这表明临床剂量的合成催产素不会从母亲转移到胎儿。
分娩时给予合成催产素输注可使产妇血浆催产素水平在最高剂量下增加 2-3 倍,与新生儿血浆催产素升高无关。因此,直接从合成催产素转移到母亲大脑或胎儿的作用不太可能。然而,分娩时给予合成催产素会改变子宫收缩模式。这可能会影响子宫血流和产妇自主神经系统活动,从而可能对胎儿造成伤害,并增加产妇的疼痛和压力。