Walker Logan C, de la Hoya Miguel, Wiggins George A R, Lindy Amanda, Vincent Lisa M, Parsons Michael T, Canson Daffodil M, Bis-Brewer Dana, Cass Ashley, Tchourbanov Alexander, Zimmermann Heather, Byrne Alicia B, Pesaran Tina, Karam Rachid, Harrison Steven, Spurdle Amanda B
Department of Pathology and Biomedical Science, University of Otago, Christchurch, New Zealand.
Molecular Oncology Laboratory, CIBERONC, Hospital Clinico San Carlos, IdISSC (Instituto de Investigación Sanitaria del Hospital Clínico San Carlos), Madrid, Spain.
medRxiv. 2023 Feb 26:2023.02.24.23286431. doi: 10.1101/2023.02.24.23286431.
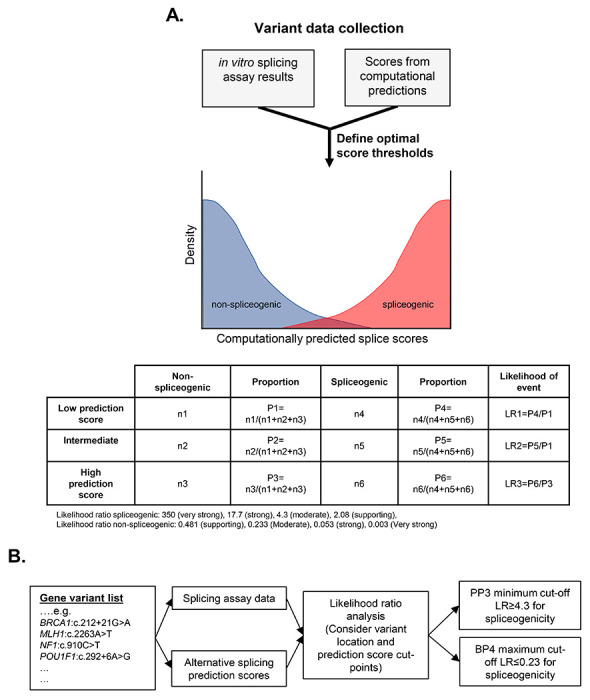
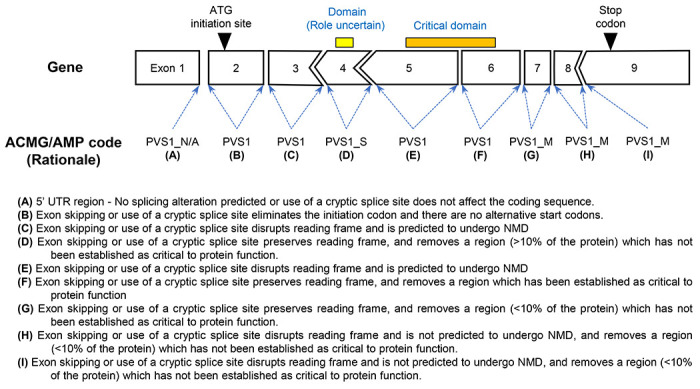
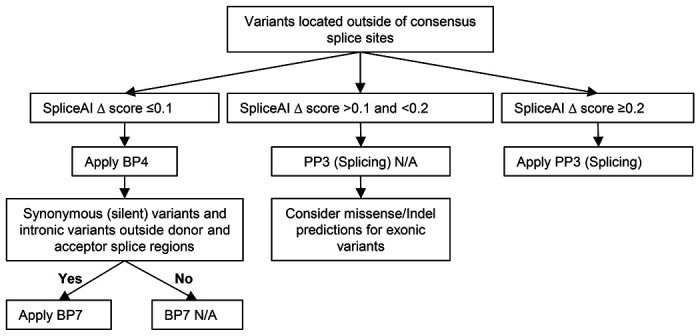
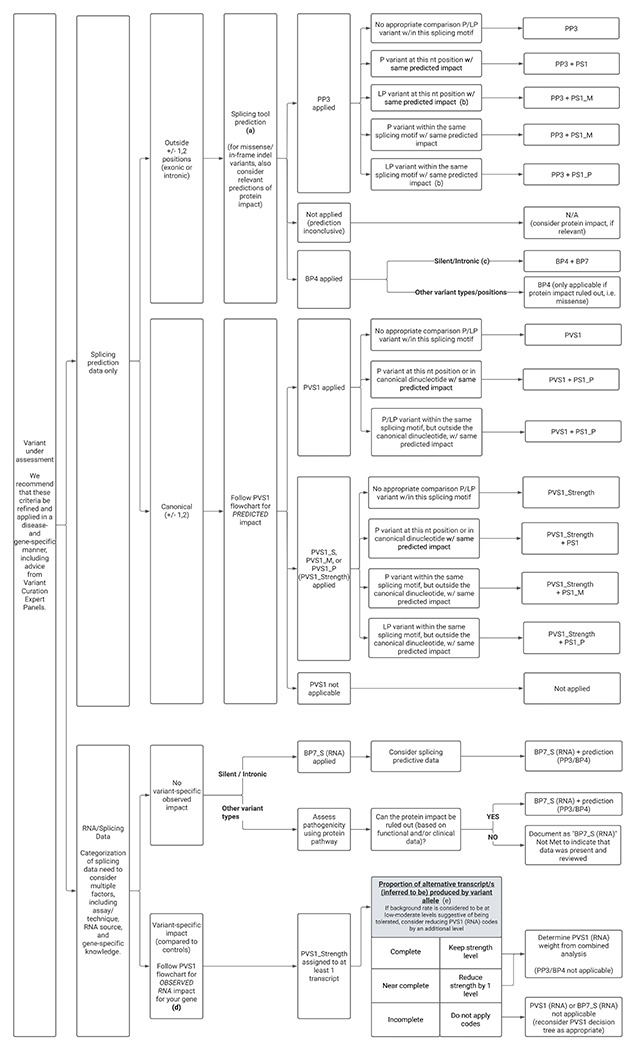
The American College of Medical Genetics and Genomics (ACMG) and the Association for Molecular Pathology (AMP) framework for classifying variants uses six evidence categories related to the splicing potential of variants: PVS1 (null variant in a gene where loss-of-function is the mechanism of disease), PS3 (functional assays show damaging effect on splicing), PP3 (computational evidence supports a splicing effect), BS3 (functional assays show no damaging effect on splicing), BP4 (computational evidence suggests no splicing impact), and BP7 (silent change with no predicted impact on splicing). However, the lack of guidance on how to apply such codes has contributed to variation in the specifications developed by different Clinical Genome Resource (ClinGen) Variant Curation Expert Panels. The ClinGen Sequence Variant Interpretation (SVI) Splicing Subgroup was established to refine recommendations for applying ACMG/AMP codes relating to splicing data and computational predictions. Our study utilised empirically derived splicing evidence to: 1) determine the evidence weighting of splicing-related data and appropriate criteria code selection for general use, 2) outline a process for integrating splicing-related considerations when developing a gene-specific PVS1 decision tree, and 3) exemplify methodology to calibrate bioinformatic splice prediction tools. We propose repurposing of the PVS1_Strength code to capture splicing assay data that provide experimental evidence for variants resulting in RNA transcript(s) with loss of function. Conversely BP7 may be used to capture RNA results demonstrating no impact on splicing for both intronic and synonymous variants, and for missense variants if protein functional impact has been excluded. Furthermore, we propose that the PS3 and BS3 codes are applied only for well-established assays that measure functional impact that is not directly captured by RNA splicing assays. We recommend the application of PS1 based on similarity of predicted RNA splicing effects for a variant under assessment in comparison to a known Pathogenic variant. The recommendations and approaches for consideration and evaluation of RNA assay evidence described aim to help standardise variant pathogenicity classification processes and result in greater consistency when interpreting splicing-based evidence.
美国医学遗传学与基因组学学会(ACMG)和分子病理学协会(AMP)的变异分类框架使用了与变异剪接潜力相关的六个证据类别:PVS1(基因中的无效变异,其中功能丧失是疾病机制)、PS3(功能测定显示对剪接有损害作用)、PP3(计算证据支持剪接效应)、BS3(功能测定显示对剪接无损害作用)、BP4(计算证据表明无剪接影响)和BP7(沉默变化,对剪接无预测影响)。然而,缺乏关于如何应用这些代码的指导导致了不同临床基因组资源(ClinGen)变异注释专家小组制定的规范存在差异。ClinGen序列变异解释(SVI)剪接亚组的成立是为了完善关于应用与剪接数据和计算预测相关的ACMG/AMP代码的建议。我们的研究利用经验性得出的剪接证据来:1)确定剪接相关数据的证据权重和一般使用的适当标准代码选择,2)概述在开发基因特异性PVS1决策树时整合剪接相关考虑因素的过程,3)举例说明校准生物信息剪接预测工具的方法。我们建议重新利用PVS1_Strength代码来获取剪接测定数据,这些数据为导致功能丧失的RNA转录本的变异提供实验证据。相反,BP7可用于获取RNA结果,表明内含子和同义变异以及错义变异(如果已排除蛋白质功能影响)对剪接均无影响。此外,我们建议仅将PS3和BS3代码应用于已确立的测定,这些测定测量的功能影响不能直接通过RNA剪接测定捕获。我们建议根据与已知致病变异相比,评估中的变异预测RNA剪接效应的相似性来应用PS1。所描述的关于考虑和评估RNA测定证据的建议和方法旨在帮助标准化变异致病性分类过程,并在解释基于剪接的证据时实现更大的一致性。