Cao Lixiu, Zhang Libo, Xu Wengui
Department of Molecular Imaging and Nuclear Medicine, Tianjin Medical University Cancer Institute and Hospital, National Clinical Research Center for Cancer, Tianjin Key Laboratory of Cancer Prevention and Therapy, Tianjin's Clinical Research Center for Cancer, Tianjin, China.
Department of Emission Computed Tomography, Tangshan People's Hospital, Tangshan, Hebei, China.
Front Oncol. 2023 Feb 8;13:1091102. doi: 10.3389/fonc.2023.1091102. eCollection 2023.
The objective of this study was to evaluate the value of biphasic contrast-enhanced computed tomography (CECT) in the differential diagnosis of metastasis and lipid-poor adenomas (LPAs) in lung cancer patients with unilateral small hyperattenuating adrenal nodule.
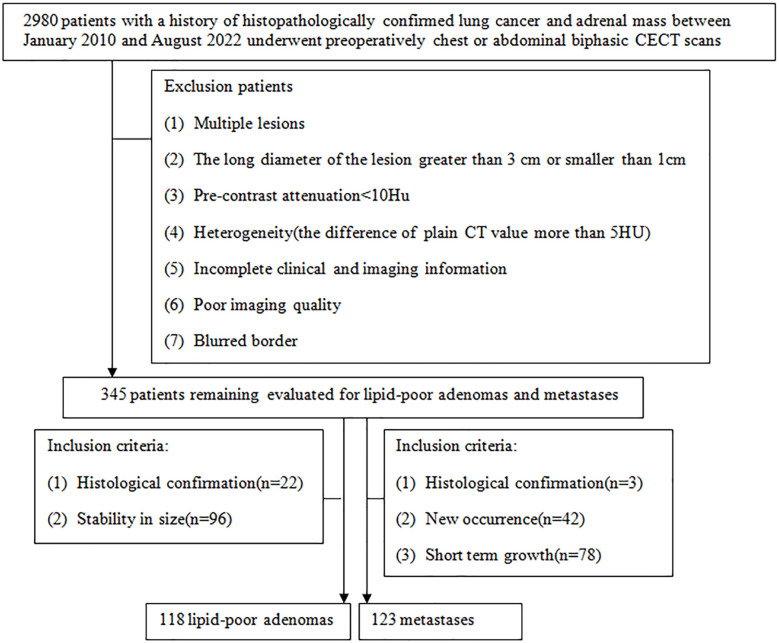
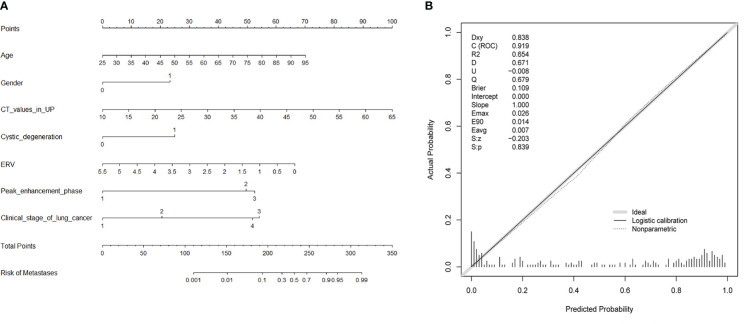
This retrospective study included 241 lung cancer patients with unilateral small hyperattenuating adrenal nodule (metastases, 123; LPAs, 118). All patients underwent plain chest or abdominal computed tomography (CT) scan and biphasic CECT scan, including arterial and venous phases. Qualitative and quantitative clinical and radiological characteristics of the two groups were compared using univariate analysis. An original diagnostic model was developed using multivariable logistic regression, and then, according to odds ratio (OR) of the risk factors of metastases, a diagnostic scoring model was developed. The areas under the receiver operating characteristic curves (AUCs) of the two diagnostic models were compared by DeLong test.
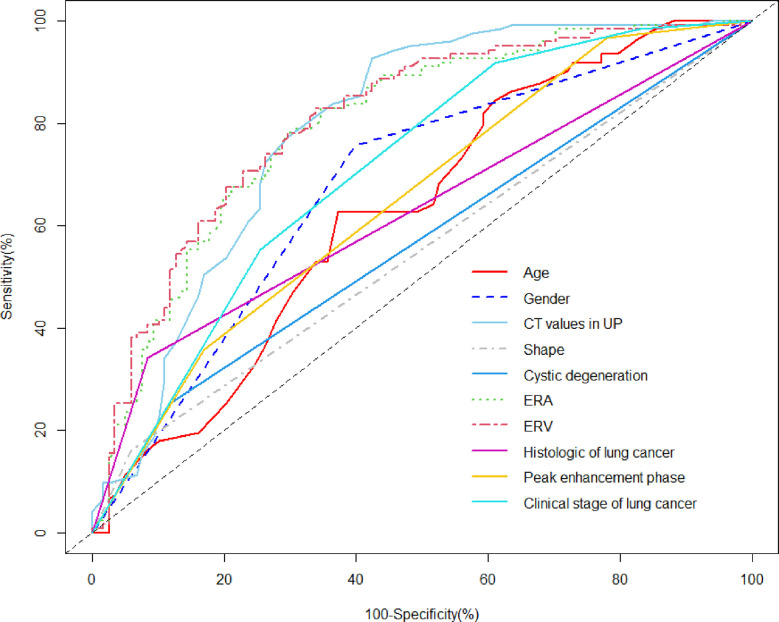
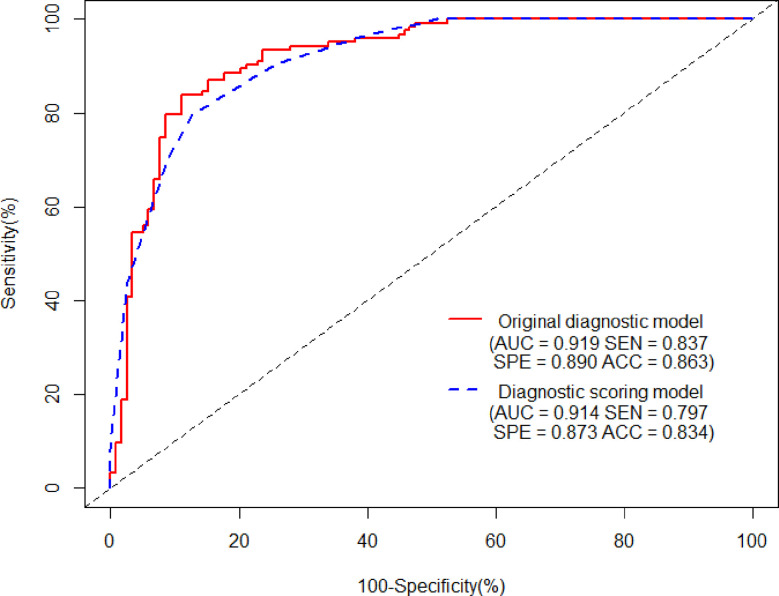
Compared with LAPs, metastases were older and showed more frequently irregular in shape and cystic degeneration/necrosis (all < 0.05). Enhancement ratios on venous (ERV) and arterial (ERA) phase of LAPs were noticeably higher than that of metastases, whereas CT values in unenhanced phase (UP) of LPAs were noticeably lower than that of metastases (all < 0.05). Compared with LAPs, the proportions of male and III/IV clinical stage and small-cell lung cancer (SCLL) were significantly higher for metastases (all < 0.05). As for peak enhancement phase, LPAs showed relatively faster wash-in and earlier wash-out enhancement pattern than metastases ( < 0.001). Multivariate analysis revealed age ≥ 59.5 years (OR: 2.269; = 0.04), male (OR: 3.511; = 0.002), CT values in UP ≥ 27.5 HU (OR: 6.968; < 0.001), cystic degeneration/necrosis (OR: 3.076; = 0.031), ERV ≤ 1.44 (OR: 4.835; < 0.001), venous phase or equally enhanced (OR: 16.907; < 0.001 or OR: 14.036; < 0.001), and clinical stage II or III or IV (OR: 3.550; = 0.208 or OR: 17.535; = 0.002 or OR: 20.241; = 0.001) were risk factors for diagnosis of metastases. AUCs of the original diagnostic model and the diagnostic scoring model for metastases were 0.919 (0.883-0.955) and 0.914 (0.880-0.948), respectively. There was no statistical significance of AUC between the two diagnostic model ( = 0.644).
Biphasic CECT performed well diagnostic ability in differentiating metastases from LAPs. The diagnostic scoring model is easy to popularize due to simplicity and convenience.
本研究旨在评估双期对比增强计算机断层扫描(CECT)在单侧肾上腺小结节强化的肺癌患者中鉴别转移瘤与乏脂性腺瘤(LPA)的价值。
本回顾性研究纳入241例单侧肾上腺小结节强化的肺癌患者(转移瘤123例,LPA 118例)。所有患者均接受胸部或腹部平扫计算机断层扫描(CT)及双期CECT扫描,包括动脉期和静脉期。采用单因素分析比较两组患者的定性和定量临床及影像学特征。利用多变量逻辑回归建立初始诊断模型,然后根据转移瘤危险因素的比值比(OR)建立诊断评分模型。通过DeLong检验比较两种诊断模型的受试者工作特征曲线下面积(AUC)。
与LPA相比,转移瘤患者年龄更大,形态不规则及囊性变/坏死更常见(均P<0.05)。LPA静脉期(ERV)和动脉期(ERA)强化率显著高于转移瘤,而LPA平扫期(UP)CT值显著低于转移瘤(均P<0.05)。与LPA相比,转移瘤患者中男性、临床分期III/IV期及小细胞肺癌(SCLL)的比例显著更高(均P<0.05)。在强化峰值期,LPA的强化模式为相对快进早出,与转移瘤不同(P<0.001)。多因素分析显示,年龄≥59.5岁(OR:2.269;P=0.04)、男性(OR:3.511;P=0.002)、UP期CT值≥27.5 HU(OR:6.968;P<0.001)、囊性变/坏死(OR:3.076;P=0.031)、ERV≤1.44(OR:4.835;P<0.001)、静脉期强化或等强化(OR:16.907;P<0.001或OR:14.036;P<0.001)以及临床分期II/III/IV期(OR:3.550;P=0.208或OR:17.535;P=0.002或OR:20.241;P=0.001)是转移瘤诊断的危险因素。转移瘤初始诊断模型和诊断评分模型的AUC分别为0.919(0.883 - 0.955)和0.914(0.880 - 0.948)。两种诊断模型的AUC差异无统计学意义(P=0.644)。
双期CECT在鉴别转移瘤与LPA方面具有良好的诊断能力。诊断评分模型因简单方便易于推广。