Asai Yuki, Arihara Hiroki, Omote Saki, Tanio Ena, Yamashita Saena, Higuchi Takashi, Hashimoto Ei, Yamada Momoko, Tsuji Hinako, Kondo Yoshihiro, Hayashi Makoto, Yamamoto Yoshiaki
Pharmacy, National Hospital Organization Mie Chuo Medical Center, 2158-5 Hisaimyojin, Tsu, Mie, 514-1101, Japan.
Pharmacy, National Hospital Organization Kanazawa Medical Center, 1-1, Shimoishibiki, Kanazawa, Ishikawa, 920-0850, Japan.
J Pharm Health Care Sci. 2023 Mar 6;9(1):10. doi: 10.1186/s40780-023-00278-x.
Polypharmacy, defined as the concurrent use of over six drugs, is common in the treatment of heart failure (HF); however, unpredictable drug interactions with bepridil may occur. In this study, we have elucidated the influence of polypharmacy on plasma bepridil concentrations in patients with HF.
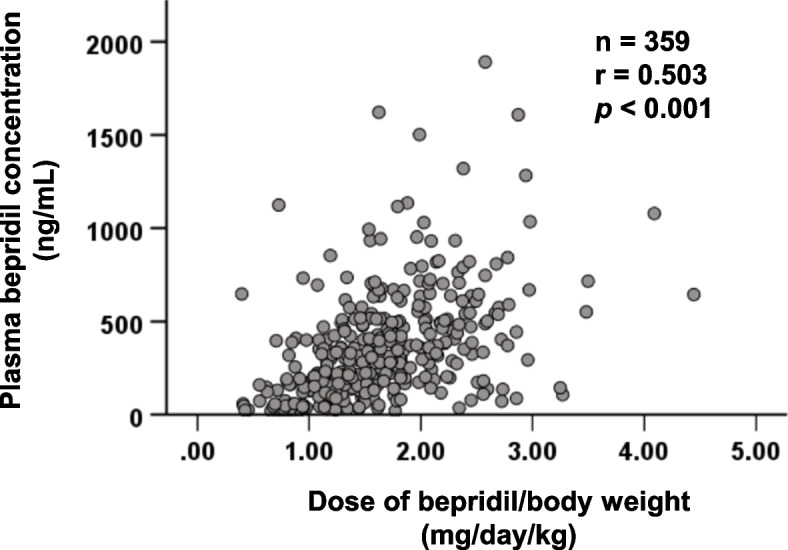
We conducted a multicenter retrospective study involving 359 adult patients with HF who received oral bepridil. Because QT prolongation is an adverse effect following plasma bepridil concentrations ≥800 ng/mL, the risk factors for patients achieving these concentrations at steady state were elucidated via multivariate logistic regression. The correlation between bepridil dose and plasma concentration was examined. The effect of polypharmacy on the value of the concentration-to-dose (C/D) ratio was investigated.
A significant relationship was observed between bepridil dose and plasma concentration (p < 0.001), and the intensity of the correlation was moderate (r = 0.503). Based on multivariate logistic regression, the adjusted odds ratios for a daily dose of bepridil ≥1.6 mg/kg, polypharmacy, and concomitant of aprindine, a cytochrome P450 2D6 inhibitor, were 6.82 (95% coefficient interval: 2.104-22.132, p = 0.001), 2.96 (95% coefficient interval: 1.014-8.643, p = 0.047), and 8.63 (95% coefficient interval: 1.684-44.215, p = 0.010), respectively. Despite the moderate correlation in non-polypharmacy, the correlation was not observed in polypharmacy. Therefore, inhibiting metabolism, along with other mechanisms, may contribute to the polypharmacy-induced increase in plasma bepridil concentrations. Moreover, the C/D ratios in the groups receiving 6-9 and 10≤ concomitant drugs were 1.28- and 1.70-fold higher than in those receiving <6 drugs, respectively.
Plasma bepridil concentrations may be influenced by polypharmacy. Moreover, the plasma bepridil concentration increased in correlation with the number of concomitant drugs used. Although the mechanism of this increase could not be determined, plasma bepridil concentrations should be periodically monitored for safe use in patients with HF.
Retrospectively registered.
多药联用被定义为同时使用超过六种药物,在心力衰竭(HF)治疗中很常见;然而,与苄普地尔可能会发生不可预测的药物相互作用。在本研究中,我们阐明了多药联用对HF患者血浆苄普地尔浓度的影响。
我们进行了一项多中心回顾性研究,纳入359例接受口服苄普地尔的成年HF患者。由于血浆苄普地尔浓度≥800 ng/mL后会出现QT间期延长这一不良反应,因此通过多因素logistic回归分析阐明患者在稳态时达到这些浓度的危险因素。研究了苄普地尔剂量与血浆浓度之间的相关性。研究了多药联用对浓度-剂量(C/D)比值的影响。
观察到苄普地尔剂量与血浆浓度之间存在显著关系(p < 0.001),且相关性强度为中等(r = 0.503)。基于多因素logistic回归分析,苄普地尔每日剂量≥1.6 mg/kg、多药联用以及同时使用细胞色素P450 2D6抑制剂阿普林定的校正比值比分别为6.82(95%置信区间:2.104 - 22.132,p = 0.001)、2.96(95%置信区间:1.014 - 8.643,p = 0.047)和8.63(95%置信区间:1.684 - 44.215,p = 0.010)。尽管在非多药联用情况下相关性为中等,但在多药联用情况下未观察到相关性。因此,除其他机制外,抑制代谢可能导致多药联用引起的血浆苄普地尔浓度升高。此外,接受6 - 9种和10种及以上联用药物组的C/D比值分别比接受少于6种药物组高1.28倍和1.70倍。
多药联用可能影响血浆苄普地尔浓度。此外,血浆苄普地尔浓度随联用药物数量的增加而升高。尽管这种升高的机制尚不能确定,但为确保HF患者安全用药,应定期监测血浆苄普地尔浓度。
回顾性注册。