Department of Rheumatology, Fukushima Medical University School of Medicine, Fukushima, Japan.
Department of Gastroenterology, Fukushima Medical University School of Medicine, Fukushima, Japan.
Front Immunol. 2023 Feb 15;14:1089492. doi: 10.3389/fimmu.2023.1089492. eCollection 2023.
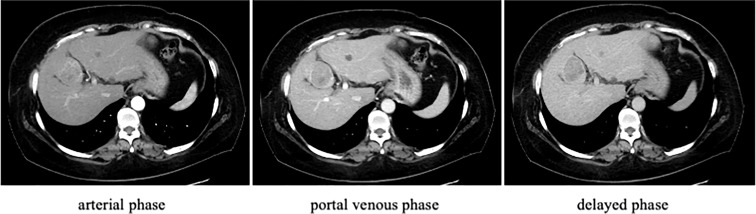
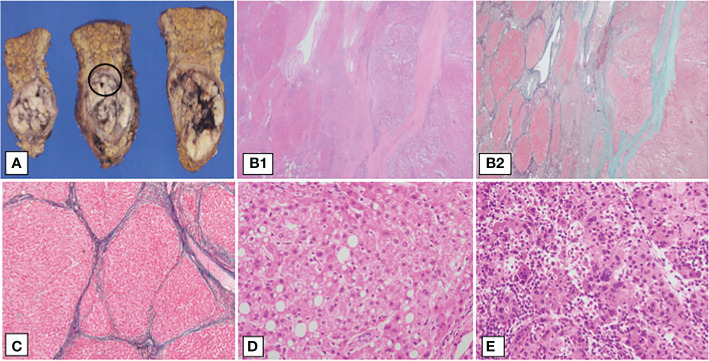
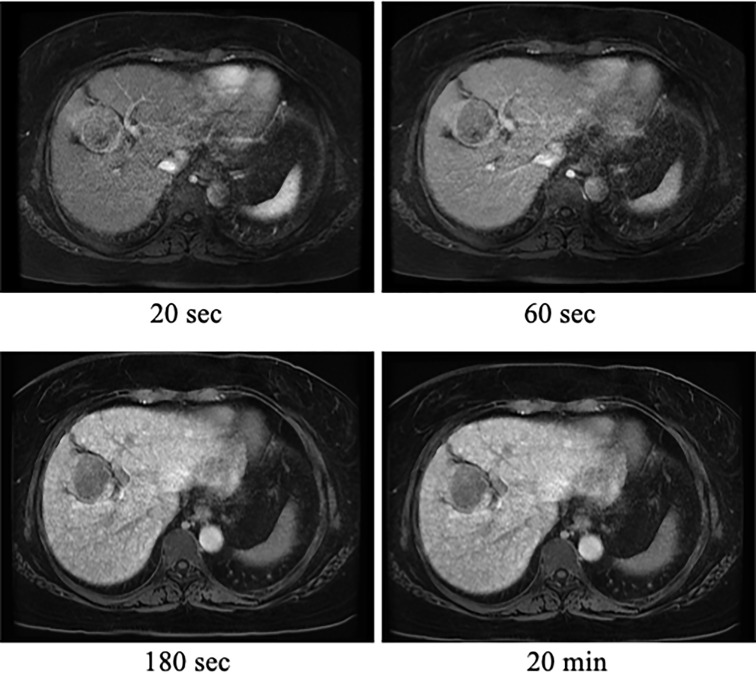
The sequential progression from chronic liver disease to cirrhosis may be a risk factor for hepatocellular carcinoma (HCC) development. Although HCC originates from hepatitis B virus- or hepatitis C virus-associated liver cirrhosis, it has recently been reported in patients with non-alcoholic steatohepatitis (NASH) with advanced fibrosis. However, little is known about the pathophysiological mechanisms linking HCC to rheumatic disorders, including rheumatoid arthritis (RA). Herein, we describe the case of HCC with NASH complicated by RA and Sjögren's syndrome (SS). A fifty-two-year-old patient with RA and diabetes was referred to our hospital for further examination of a liver tumor. She received methotrexate (4 mg/week) for 3 years and adalimumab (40 mg/biweekly) for 2 years. On admission, laboratory data showed mild thrombocytopenia and hypoalbuminemia, with normal hepatitis virus markers or liver enzymes. Anti-nuclear antibodies were positive with high titers (x640), and anti-SS-A/Ro (187.0 U/ml; normal range [NR]: ≤6.9 U/mL) and anti-SS-B/La (320 U/ml; NR: ≤6.9 U/mL) antibodies were also high. Abdominal ultrasonography and computed tomography revealed liver cirrhosis and a tumor in the left lobe (S4) of the liver. She was diagnosed with HCC based on imaging findings, and elevated levels of protein induced by vitamin K absence- II (PIVKA-II) were detected. She underwent laparoscopic partial hepatectomy, and histopathological examination revealed steatohepatitis HCC with background liver cirrhosis. The patient was discharged on the 8 day post-operation without any complications. At the 30 months follow-up, no significant evidence of recurrence was observed. Our case suggests that clinical screening for HCC is needed in patients with RA who are at a high risk of NASH, as they may progress to HCC even without elevated liver enzymes.
慢性肝病向肝硬化的连续进展可能是肝细胞癌(HCC)发展的一个危险因素。尽管 HCC 起源于乙型肝炎病毒或丙型肝炎病毒相关的肝硬化,但最近在伴有晚期纤维化的非酒精性脂肪性肝炎(NASH)患者中也有报道。然而,对于将 HCC 与包括类风湿关节炎(RA)在内的风湿性疾病联系起来的病理生理机制知之甚少。在此,我们描述了一例伴有 NASH 的 HCC 合并 RA 和干燥综合征(SS)的病例。一位 52 岁的 RA 合并糖尿病患者因肝肿瘤到我院进一步检查。她接受了 3 年的甲氨蝶呤(4mg/周)和 2 年的阿达木单抗(40mg/每两周)治疗。入院时,实验室数据显示血小板轻度减少和低白蛋白血症,肝炎病毒标志物或肝酶正常。抗核抗体阳性,滴度较高(x640),抗 SS-A/Ro(187.0U/ml;正常值[NR]:≤6.9U/ml)和抗 SS-B/La(320U/ml;NR:≤6.9U/ml)抗体也升高。腹部超声和计算机断层扫描显示肝硬化和肝左叶(S4)的肿瘤。根据影像学表现诊断为 HCC,并检测到维生素 K 缺乏诱导蛋白 II(PIVKA-II)水平升高。她接受了腹腔镜部分肝切除术,组织病理学检查显示背景肝硬化的脂肪性肝炎 HCC。患者术后第 8 天无并发症出院。在 30 个月的随访中,未观察到明显的复发迹象。我们的病例表明,RA 患者患 NASH 的风险较高,因此即使肝酶没有升高,也需要进行 HCC 的临床筛查。