Department of Oral Pathology and Medicine, University of Benin, 302001 Edo State, Nigeria.
Research Department, Institute of Human Virology, Nigeria, 900107 Abuja, Nigeria.
J Clin Pediatr Dent. 2023 Mar;47(2):1-9. doi: 10.22514/jocpd.2023.007. Epub 2023 Mar 3.
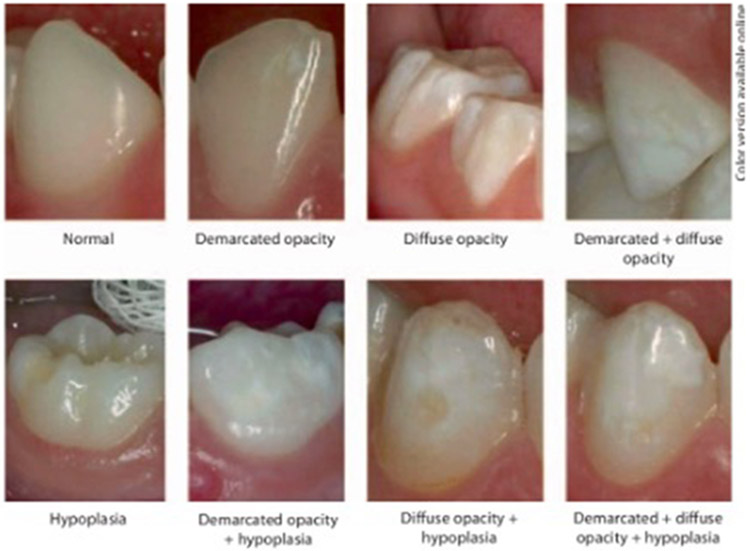
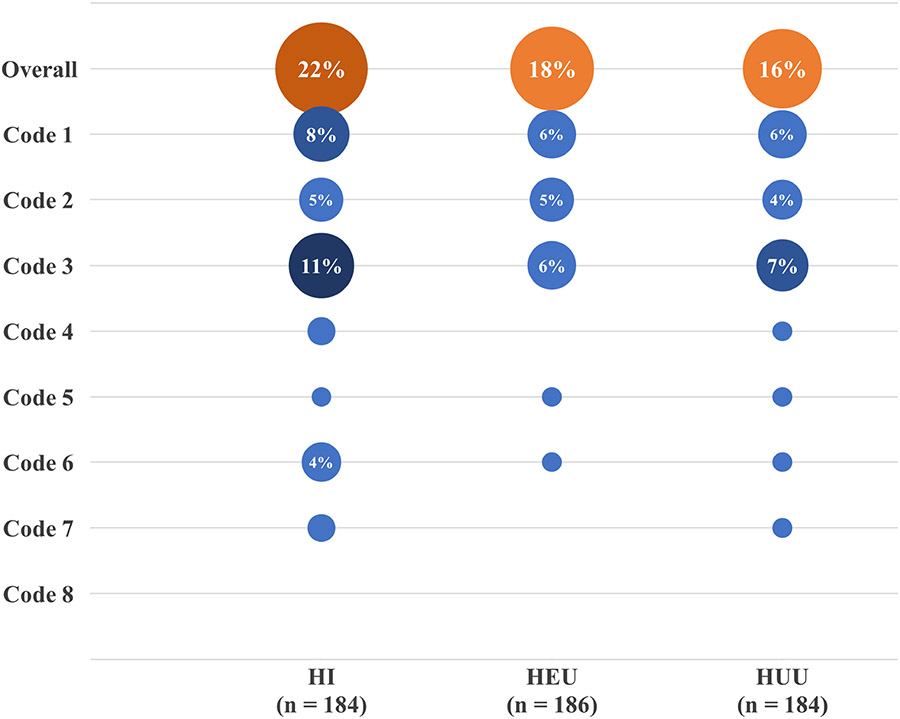
To evaluate the prevalence and pattern of developmental defects of the enamel (DDE) and their risk factors among children born infected with Human Immunodeficiency Virus (HIV) and those born to HIV-infected mothers compared with their unexposed counterparts (, children born to uninfected mothers). This was an analytic cross-sectional study evaluating the presence and pattern of distribution of DDE in three groups of school-aged children (age, 4-11 years) receiving care and treatment at a Nigerian tertiary hospital, comprising: (1) HIV-infected (HI) on antiretroviral therapy (ART) (n = 184), (2) HIV-exposed but uninfected (HEU) (n = 186) and (3) HIV-unexposed and uninfected (HUU) (n = 184). Data capture forms and questionnaires were used to record the children's medical and dental history based on clinical chart review and recall from their parents/guardians. Dental examinations were performed by calibrated dentists blinded to the study grouping. CD4+ (Cluster of Differentiation) T-cell counts were assayed for all participants. The diagnosis of DDE corresponded with the codes enumerated in the World Dental Federation's modified DDE Index. Analyses relied on comparative statistics to determine risk factors associated with DDE. A total of 103 participants distributed among the three groups presented with at least one form of DDE, which indicated a prevalence of 18.59%. The HI group had the highest frequency of DDE-affected teeth (4.36%), while that of the HEU and HUU groups were 2.73% and 2.05%, respectively. Overall, the most encountered DDE was code 1 (Demarcated Opacity), accounting for 30.93% of all codes. DDE codes 1, 4 and 6 showed significant associations with the HI and HEU groups in both dentitions ( < 0.05). We found no significant association DDE and either very low birth weight or preterm births. A marginal association with CD4+ lymphocyte count was observed in HI participants. DDE is prevalent in school-aged children, and HIV infection is a significant risk factor for hypoplasia, a common form of DDE. Our results were consistent with other research linking controlled HIV (with ART) to oral diseases and reinforce advocacies for public policies targeted at infants exposed/infected perinatally with HIV.
评估在感染人类免疫缺陷病毒(HIV)的儿童和感染 HIV 的母亲所生儿童(HIV 暴露但未感染的儿童)与未暴露的对照组(未感染的母亲所生儿童)中,发育性牙釉质缺陷(DDE)的流行率和模式及其危险因素。这是一项分析性横断面研究,评估了在尼日利亚一家三级医院接受治疗的三组学龄儿童(年龄 4-11 岁)中 DDE 的存在和分布模式:(1)接受抗逆转录病毒治疗(ART)的 HIV 感染(HI)(n=184),(2)HIV 暴露但未感染(HEU)(n=186)和(3)HIV 未暴露且未感染(HUU)(n=184)。数据采集表和问卷用于根据临床图表审查和从父母/监护人处回忆记录儿童的医疗和牙科史。由经过校准的牙医进行牙科检查,他们对研究分组不知情。对所有参与者进行 CD4+(分化簇)T 细胞计数。DDE 的诊断与世界牙科联合会修改后的 DDE 指数中列举的代码相对应。分析依赖于比较统计学来确定与 DDE 相关的危险因素。共有 103 名参与者分布在三组中,至少有一种形式的 DDE,患病率为 18.59%。HI 组 DDE 受累牙齿的频率最高(4.36%),而 HEU 和 HUU 组分别为 2.73%和 2.05%。总体而言,最常见的 DDE 是代码 1(有界不透明),占所有代码的 30.93%。DDE 代码 1、4 和 6 在两个牙列中均与 HI 和 HEU 组显著相关(<0.05)。我们没有发现 DDE 与极低出生体重或早产之间有显著关联。在 HI 参与者中观察到与 CD4+淋巴细胞计数有边缘关联。DDE 在学龄儿童中很常见,HIV 感染是发育不良的一个重要危险因素,发育不良是 DDE 的常见形式。我们的结果与其他将受控制的 HIV(使用 ART)与口腔疾病联系起来的研究一致,并加强了针对围产期感染 HIV 的婴儿的公共政策宣传。