Department of Liver Surgery and Transplantation, Liver Cancer Institute, Zhongshan Hospital, Fudan University, Shanghai, China.
Key Laboratory of Carcinogenesis and Cancer Invasion, Ministry of Education, Fudan University, Shanghai, China.
Front Immunol. 2023 Feb 23;14:1141199. doi: 10.3389/fimmu.2023.1141199. eCollection 2023.
Lenvatinib monotherapy and combination therapy with immune checkpoint inhibitors (ICI) were widely applied for unresectable hepatocellular carcinoma (uHCC). However, many patients failed to benefit from the treatments. A prognostic model was needed to predict the treatment outcomes and guide clinical decisions.
304 patients receiving lenvatinib monotherapy or lenvatinib plus ICI for uHCC were retrospectively included. The risk factors derived from the multivariate analysis were used to construct the predictive model. The C-index and area under the receiver-operating characteristic curve (AUC) were calculated to assess the predictive efficiency.
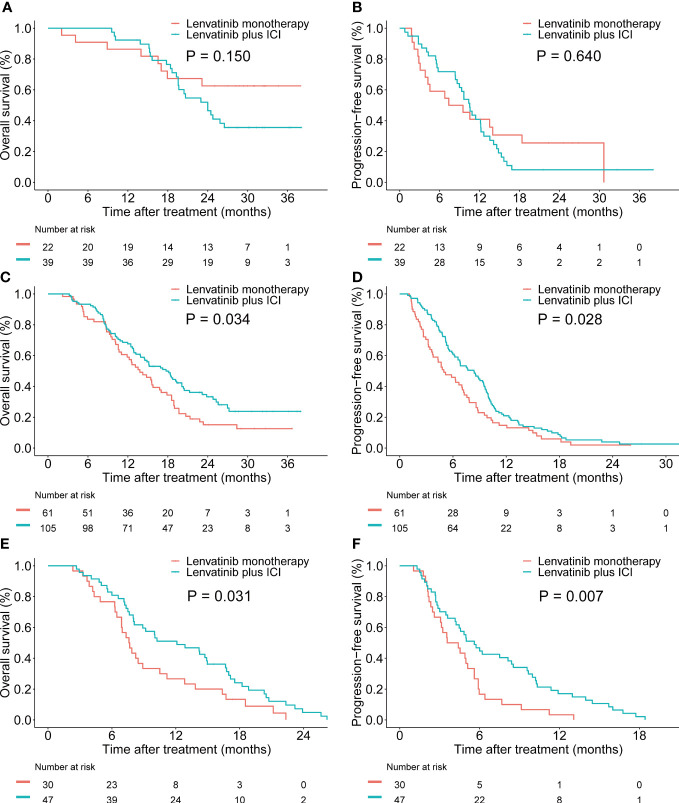
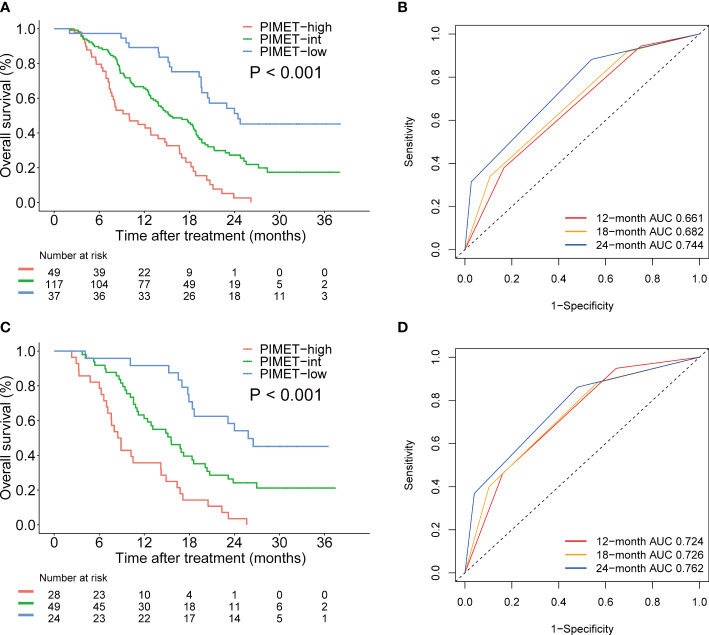
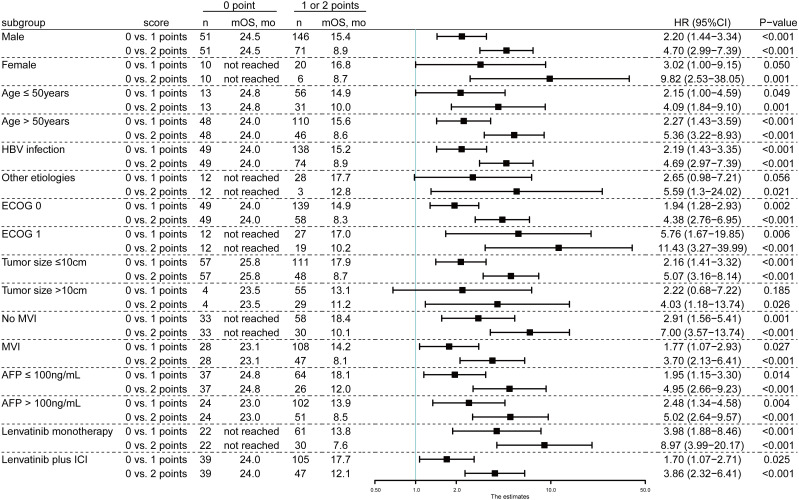
Multivariate analysis revealed that protein induced by vitamin K absence or antagonist-II (PIVKA-II) (HR, 2.05; P=0.001) and metastasis (HR, 2.07; P<0.001) were independent risk factors of overall survival (OS) in the training cohort. Herein, we constructed a prognostic model called PIMET score and stratified patients into the PIMET-low group (without metastasis and PIVKA-II<600 mAU/mL), PIMET-int group (with metastasis or PIVKA-II>600 mAU/mL) and PIMET-high group (with metastasis and PIVKA-II>600 mAU/mL). The C-index of PIMET score for the survival prediction was 0.63 and 0.67 in the training and validation cohort, respectively. In the training cohort, the AUC of 12-, 18-, and 24-month OS was 0.661, 0.682, and 0.744, respectively. The prognostic performances of the model were subsequently validated. The AUC of 12-, 18-, and 24-month OS was 0.724, 0.726, and 0.762 in the validation cohort. Subgroup analyses showed consistent predictive value for patients receiving lenvatinib monotherapy and patients receiving lenvatinib plus ICI. The PIMET score could also distinguish patients with different treatment responses. Notably, the combination of lenvatinib and ICI conferred survival benefits to patients with PIMET-int or PIMET-high, instead of patients with PIMET-low.
The PIMET score comprising metastasis and PIVKA-II could serve as a helpful prognostic model for uHCC receiving lenvatinib monotherapy or lenvatinib plus ICI. The PIMET score could guide the treatment decision and facilitate precision medicine for uHCC patients.
仑伐替尼单药治疗和联合免疫检查点抑制剂(ICI)治疗已广泛用于不可切除的肝细胞癌(uHCC)。然而,许多患者并未从中受益。因此需要建立一个预测模型来预测治疗结果并指导临床决策。
回顾性纳入 304 例接受仑伐替尼单药或仑伐替尼联合 ICI 治疗的 uHCC 患者。从多变量分析中得出的风险因素用于构建预测模型。计算 C 指数和接受者操作特征曲线下的面积(AUC)以评估预测效率。
多变量分析显示,维生素 K 缺乏或拮抗剂 II 诱导蛋白(PIVKA-II)(HR,2.05;P=0.001)和转移(HR,2.07;P<0.001)是训练队列中总生存期(OS)的独立危险因素。在此基础上,我们构建了一个称为 PIMET 评分的预后模型,并将患者分为 PIMET-低组(无转移和 PIVKA-II<600 mAU/mL)、PIMET-中组(有转移或 PIVKA-II>600 mAU/mL)和 PIMET-高组(有转移和 PIVKA-II>600 mAU/mL)。PIMET 评分用于生存预测的 C 指数在训练和验证队列中分别为 0.63 和 0.67。在训练队列中,12、18 和 24 个月 OS 的 AUC 分别为 0.661、0.682 和 0.744。随后验证了该模型的预测性能。在验证队列中,12、18 和 24 个月 OS 的 AUC 分别为 0.724、0.726 和 0.762。亚组分析表明,该模型对接受仑伐替尼单药治疗和接受仑伐替尼联合 ICI 治疗的患者均具有一致的预测价值。PIMET 评分还可以区分不同治疗反应的患者。值得注意的是,仑伐替尼联合 ICI 为 PIMET-中或 PIMET-高的患者带来了生存获益,而不是 PIMET-低的患者。
包含转移和 PIVKA-II 的 PIMET 评分可作为接受仑伐替尼单药治疗或仑伐替尼联合 ICI 治疗的 uHCC 的有用预后模型。PIMET 评分可以指导治疗决策并促进 uHCC 患者的精准医学。