Engelhart Alexis, Mason Stacey, Nwaozuru Ucheoma, Obiezu-Umeh Chisom, Carter Victoria, Shato Thembekile, Gbaja-Biamila Titilola, Oladele David, Iwelunmor Juliet
Department of Behavioral Science and Health Education, College for Public Health and Social Justice, Saint Louis University, Saint Louis, MO, United States.
Department of Implementation Science, Wake Forest School of Medicine, Winston-Salem, NC, United States.
Front Health Serv. 2022 Aug 11;2:889390. doi: 10.3389/frhs.2022.889390. eCollection 2022.
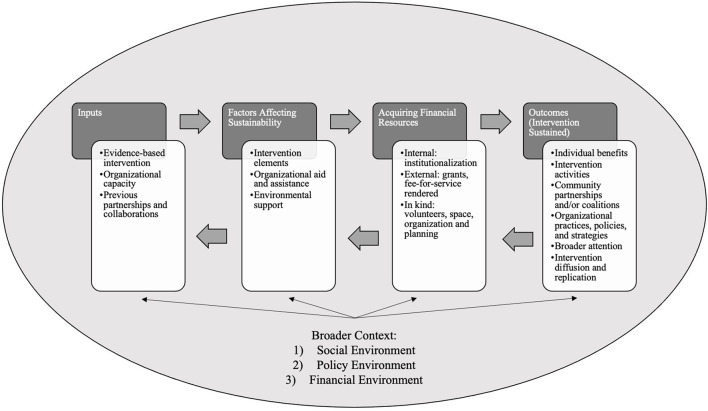
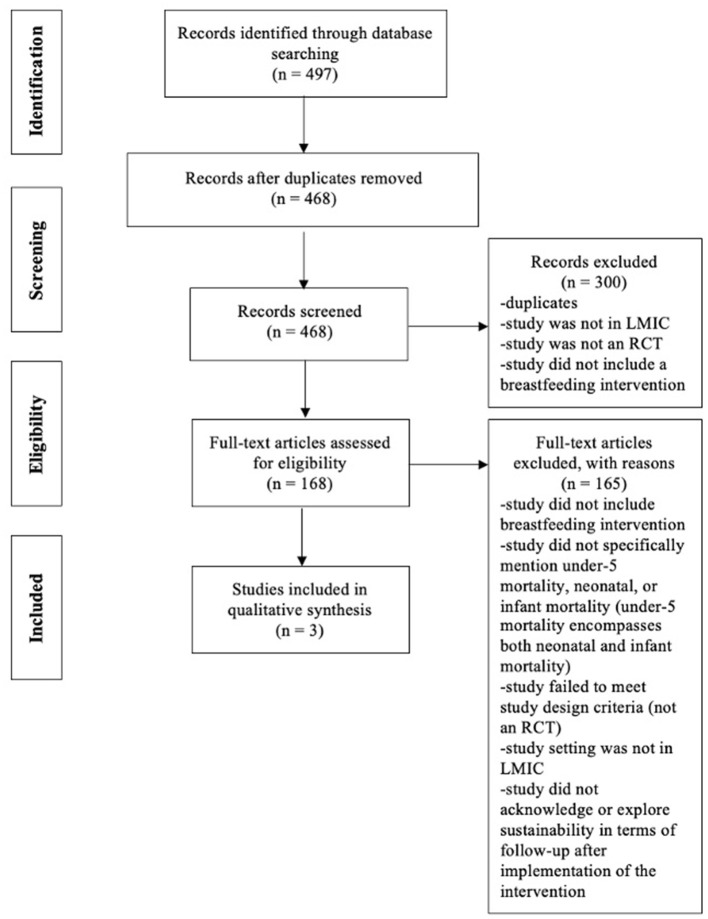
Child mortality is the lowest it has ever been, but the burden of death in low- and middle-income countries (LMICs) is still prevalent, and the numbers average above the global mean. Breastfeeding contributes to the reduction of child mortality by improving chance of survival beyond childhood. Therefore, it is essential to examine how evidence-based breastfeeding interventions are being maintained in resource-constrained settings. Guided by Scheirer and Dearing's sustainability framework, the aim of this systematic review was to explore how evidence-based breastfeeding interventions implemented to address child mortality in LMICs are sustained. The literature search included randomized controlled trials (RCTs) of breastfeeding interventions from the following electronic databases: Cochrane Library, Global Health, PubMed, Scopus, and Web of Science. Literature selection and data extraction were completed according to the PRISMA guidelines. A narrative synthesis was used to investigate factors that contributed to sustainability failure or success. A total of 497 articles were identified through the database search. Only three papers were included in the review after the removal of duplicates and assessment for eligibility. The three RCTs included breastfeeding interventions predominately focusing on breastfeeding initiation and exclusivity in rural, semi-rural, and peri-urban areas in South Africa, Kenya, and India. The number of women included in the studies ranged from 901 to 3,890, and the duration of studies stretched from 6 weeks to 2.5 years. In two studies, sustainability was reported as the continuation of the intervention, and the other study outlined program dissemination and scale-up. Facilitators and barriers that influenced the sustainability of breastfeeding interventions were largely related to specific characteristics of the interventions (i.e., strong intervention implementers-facilitator; small number of CHWs involved-barrier). Optimizing the sustainability of breastfeeding interventions in LMICs is imperative to reduce child mortality. The focal point of implementation must be planning for sustainability to lead to continued benefits and changes in population outcomes. A defined action plan for sustainability needs to be included in both funding and research.
儿童死亡率处于历史最低水平,但低收入和中等收入国家(LMICs)的死亡负担仍然普遍存在,且平均数字高于全球平均水平。母乳喂养通过提高儿童期后存活的几率,有助于降低儿童死亡率。因此,研究在资源有限的环境中如何维持基于证据的母乳喂养干预措施至关重要。在谢勒和迪林的可持续性框架指导下,本系统评价的目的是探讨为解决LMICs儿童死亡率而实施的基于证据的母乳喂养干预措施是如何得以维持的。文献检索包括来自以下电子数据库的母乳喂养干预随机对照试验(RCTs):考科蓝图书馆、全球健康、医学期刊数据库、Scopus和科学网。文献筛选和数据提取按照系统评价和Meta分析的首选报告项目(PRISMA)指南完成。采用叙述性综合分析来研究导致可持续性失败或成功的因素。通过数据库检索共识别出497篇文章。在去除重复项并评估 eligibility 后,综述仅纳入了三篇论文。这三项RCTs包括的母乳喂养干预主要集中在南非、肯尼亚和印度的农村、半农村和城郊地区的母乳喂养启动和纯母乳喂养。研究纳入的女性数量从901人到3890人不等,研究持续时间从6周到2.5年。在两项研究中,可持续性被报告为干预措施的延续,另一项研究概述了项目传播和扩大规模的情况。影响母乳喂养干预可持续性的促进因素和障碍在很大程度上与干预措施的具体特征有关(即强有力的干预实施者——促进因素;参与的社区卫生工作者数量少——障碍)。优化LMICs母乳喂养干预措施的可持续性对于降低儿童死亡率至关重要。实施的重点必须是为可持续性进行规划,以带来持续的益处并改变人群结果。在资金和研究中都需要纳入明确的可持续性行动计划。