Department of General and Interventional Cardiology, Heart and Diabetes Center North Rhine-Westphalia Ruhr University Bochum Bad Oeynhausen Germany.
First Department of Medicine, Klinikum rechts der Isar Technical University of Munich Munich Germany.
J Am Heart Assoc. 2023 Mar 21;12(6):e028737. doi: 10.1161/JAHA.122.028737. Epub 2023 Mar 16.
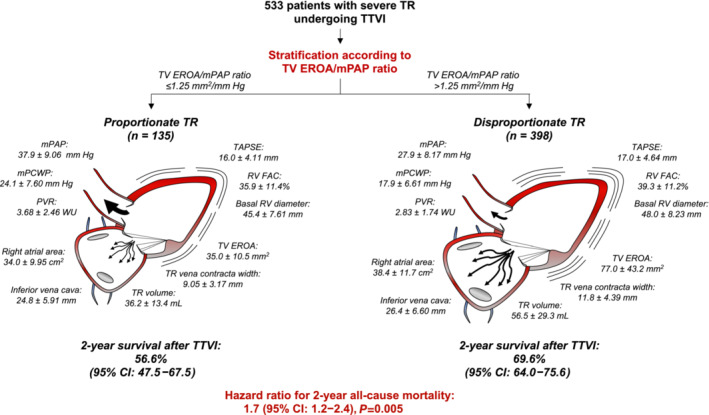
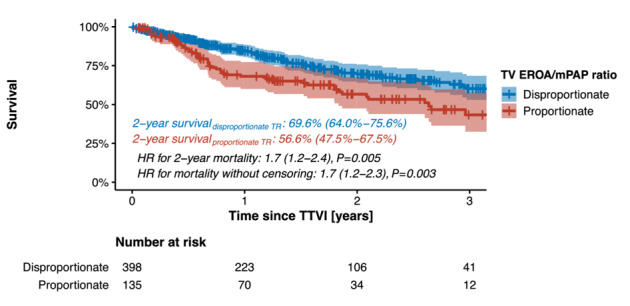
Background Tricuspid regurgitation (TR) frequently develops in patients with long-standing pulmonary hypertension, and both pathologies are associated with increased morbidity and mortality. This study aimed to improve prognostic assessment in patients with severe TR undergoing transcatheter tricuspid valve intervention (TTVI) by relating the extent of TR to pulmonary artery pressures. Methods and Results In this multicenter study, we included 533 patients undergoing TTVI for moderate-to-severe or severe TR. The proportionality framework was based on the ratio of tricuspid valve effective regurgitant orifice area to mean pulmonary artery pressure. An optimal threshold for tricuspid valve effective regurgitant orifice area/mean pulmonary artery pressure ratio was derived on 353 patients with regard to 2-year all-cause mortality and externally validated on 180 patients. Patients with a tricuspid valve effective regurgitant orifice area/mean pulmonary artery pressure ratio ≤1.25 mm/mm Hg (defining proportionate TR) featured significantly lower 2-year survival rates after TTVI than patients with disproportionate TR (56.6% versus 69.6%; =0.005). In contrast with patients with disproportionate TR (n=398), patients with proportionate TR (n=135) showed more pronounced mPAP levels (37.9±9.06 mm Hg versus 27.9±8.17 mm Hg; <2.2×10) and more severely impaired right ventricular function (tricuspid annular plane systolic excursion: 16.0±4.11 versus 17.0±4.64 mm; =0.012). Moreover, tricuspid valve effective regurgitant orifice area was smaller in patients with proportionate TR when compared with disproportionate TR (0.350±0.105 cm versus 0.770±0.432 cm; <2.2×10). Importantly, proportionate TR remained a significant predictor for 2-year mortality after adjusting for demographic and clinical variables (hazard ratio, 1.7; =0.006). Conclusions The proposed proportionality framework promises to improve future risk stratification and clinical decision-making by identifying patients who benefit the most from TTVI (disproportionate TR). As a next step, randomized controlled studies with a conservative treatment arm are needed to quantify the net benefit of TTVI in patients with proportionate TR.
三尖瓣反流(TR)在长期肺动脉高压患者中经常发生,这两种病理都与发病率和死亡率增加有关。本研究旨在通过将 TR 程度与肺动脉压相关联,来改善接受经导管三尖瓣瓣膜介入治疗(TTVI)的严重 TR 患者的预后评估。
在这项多中心研究中,我们纳入了 533 例接受 TTVI 治疗的中重度或重度 TR 患者。比例框架基于三尖瓣有效反流口面积与平均肺动脉压的比值。在 353 例患者中,根据 2 年全因死亡率得出了三尖瓣有效反流口面积/平均肺动脉压比值的最佳阈值,并在 180 例患者中进行了外部验证。三尖瓣有效反流口面积/平均肺动脉压比值≤1.25mm/mm Hg(定义为比例性 TR)的患者在 TTVI 后 2 年生存率显著低于非比例性 TR 患者(56.6% vs. 69.6%;=0.005)。与非比例性 TR 患者(n=398)相比,比例性 TR 患者(n=135)的 mPAP 水平更高(37.9±9.06mm Hg 与 27.9±8.17mm Hg;<2.2×10),右心室功能受损更严重(三尖瓣环平面收缩期位移:16.0±4.11mm 与 17.0±4.64mm;=0.012)。此外,与非比例性 TR 患者相比,比例性 TR 患者的三尖瓣有效反流口面积更小(0.350±0.105cm 与 0.770±0.432cm;<2.2×10)。重要的是,在调整人口统计学和临床变量后,比例性 TR 仍然是 2 年死亡率的显著预测因子(危险比,1.7;=0.006)。
所提出的比例框架有望通过识别最受益于 TTVI(非比例性 TR)的患者来改善未来的风险分层和临床决策。下一步,需要进行具有保守治疗组的随机对照研究,以量化 TTVI 在比例性 TR 患者中的净获益。