Department of Gynecology and Obstetrics, Máxima Medical Centre, De Run 4600, 5500 MB, Veldhoven, The Netherlands.
GROW, Research School of Oncology and Developmental Biology, University of Maastricht, Universiteitssingel 40, 6229 ER, Maastricht, The Netherlands.
BMC Womens Health. 2023 Mar 21;23(1):115. doi: 10.1186/s12905-023-02286-3.
The aim of this study was to describe the natural course of pelvic floor symptoms and pelvic floor anatomy for women long-term after hysterectomy.
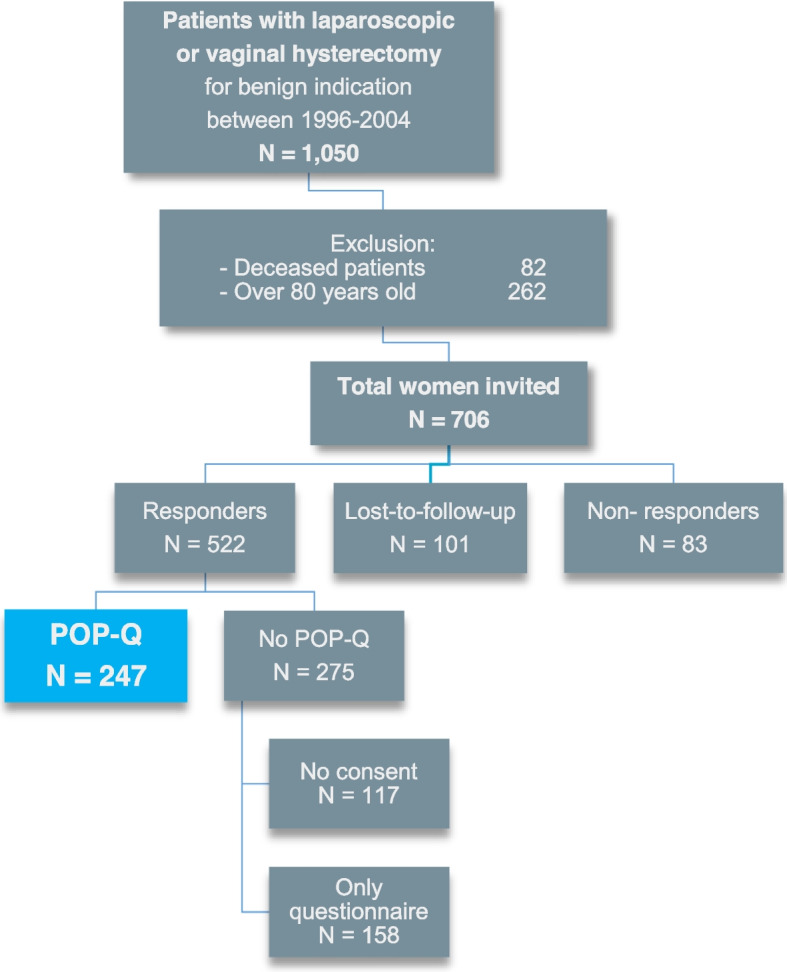
Women who underwent hysterectomy between 1996-2004 carried out the PFDI-20 questionnaire and POP-Q examination. We collected data on the presence and type of pelvic floor symptoms and its relation to the degree of pelvic organ prolapse (POP) per compartment (≥ stage 2).
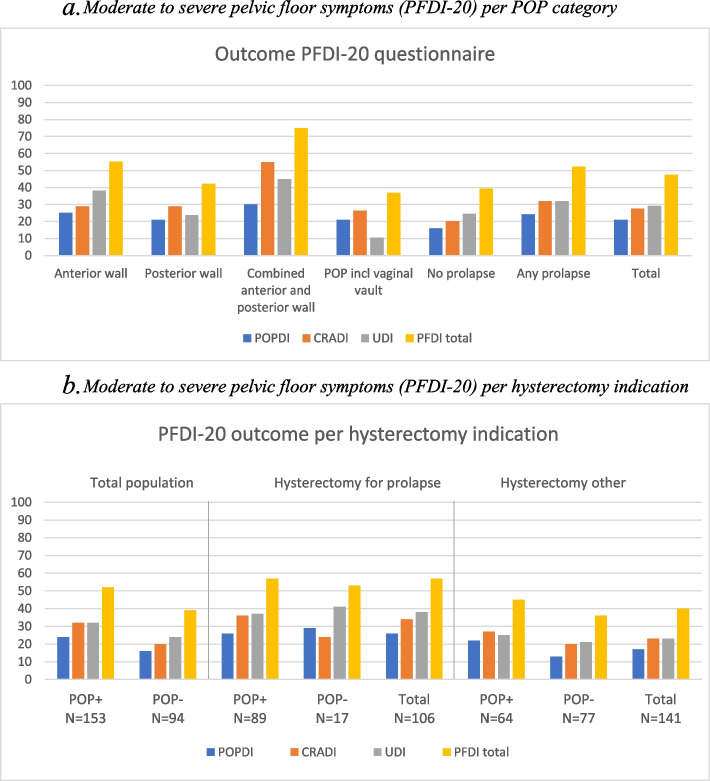
We obtained data from 247 women on average sixteen years after hysterectomy, with no prolapse (n = 94), anterior prolapse (n = 76), posterior prolapse (n = 38), both anterior- and posterior prolapse (n = 20), and a prolapse involving the vaginal vault (n = 19). Of all 153 women with ≥ stage 2 prolapse, 80 (52%) experienced moderate and/or severe symptoms of the PFDI-20. Most frequently reported symptoms by women with POP were uncontrollable flatus, urinary frequency and urge incontinence. Bulging was associated with a prolapse beyond the hymen. 39% Of women without prolapse experienced bothersome pelvic floor symptoms as well. Most often these were stress incontinence, straining to pass stool and incomplete bowel emptying. Women with a history of hysterectomy for prolapse have more pelvic floor symptoms than women who underwent hysterectomy for other indications, regardless of the current presence of POP (57% versus 40%, p = 0.009).
In a group of post-hysterectomy women who did not actively seek help, 47% experienced problematic pelvic floor symptoms, independent of the presence or absence of an anatomic POP. Creating more knowledge and awareness of the impact of hysterectomy on the pelvic floor can help women in the future.
The study was registered in the Dutch Trial Registry; Trial NL5967 (NTR6333, 2017-02-01) and approved by the Medical Research Ethics Committee of the Máxima Medical Center (NL60096.015.16, 2017-02-24).
本研究旨在描述子宫切除术后女性盆底症状和盆底解剖结构的自然病程。
1996 年至 2004 年间接受子宫切除术的女性完成了 PFDI-20 问卷和 POP-Q 检查。我们收集了盆底症状的存在和类型的数据,并将其与每个隔室(≥阶段 2)的盆腔器官脱垂(POP)程度相关联。
我们平均在子宫切除术后 16 年获得了 247 名女性的数据,无脱垂(n=94)、前位脱垂(n=76)、后位脱垂(n=38)、前位和后位脱垂(n=20)以及阴道穹隆脱垂(n=19)。在所有 153 名≥2 期脱垂的女性中,80 名(52%)报告了 PFDI-20 的中度和/或重度症状。POP 女性最常报告的症状是无法控制的放屁、尿频和急迫性尿失禁。膨出与处女膜外的脱垂有关。93%无脱垂的女性也经历了烦人的盆底症状。最常见的是压力性尿失禁、排便费力和不完全排空。因脱垂而接受子宫切除术的女性比因其他原因接受子宫切除术的女性有更多的盆底症状,无论当前是否存在 POP(57%比 40%,p=0.009)。
在一组未主动寻求帮助的子宫切除术后女性中,47%的人出现了有问题的盆底症状,与是否存在解剖学 POP 无关。增加对子宫切除术对盆底影响的认识可以帮助未来的女性。
该研究在荷兰试验注册中心注册;试验 NL5967(NTR6333,2017-02-01),并获得了马克西玛医疗中心医学伦理委员会的批准(NL60096.015.16,2017-02-24)。