Wang Lei, Li Chunxing, Zhao Zichen, Li Xiaojian, Tang Chong, Guan Zhenpeng, Sun Feng, Gu Jin, Li Ningchen
Wu Jieping Urology Center, Peking University Shougang Hospital, Beijing, China.
Department of Pharmacy, Aerospace Center Hospital, Beijing, China.
Front Oncol. 2023 Mar 7;13:1104242. doi: 10.3389/fonc.2023.1104242. eCollection 2023.
The best choice of first-line treatment for metastatic hormone-sensitive prostate cancer (mHSPC) is unclear. We aimed to compare the effectiveness and safety determined in randomized clinical trials of doublet and triplet treatments for mHSPC.
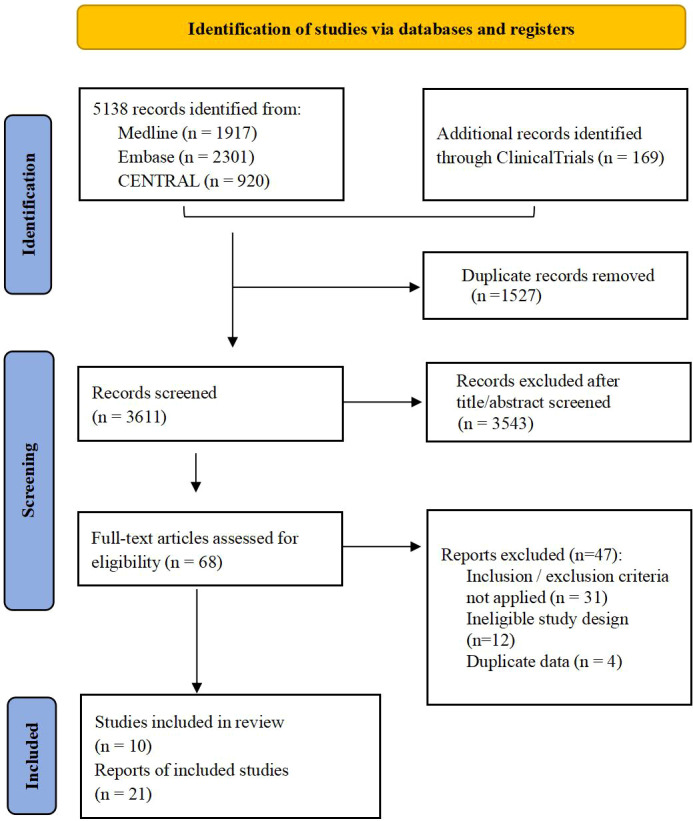
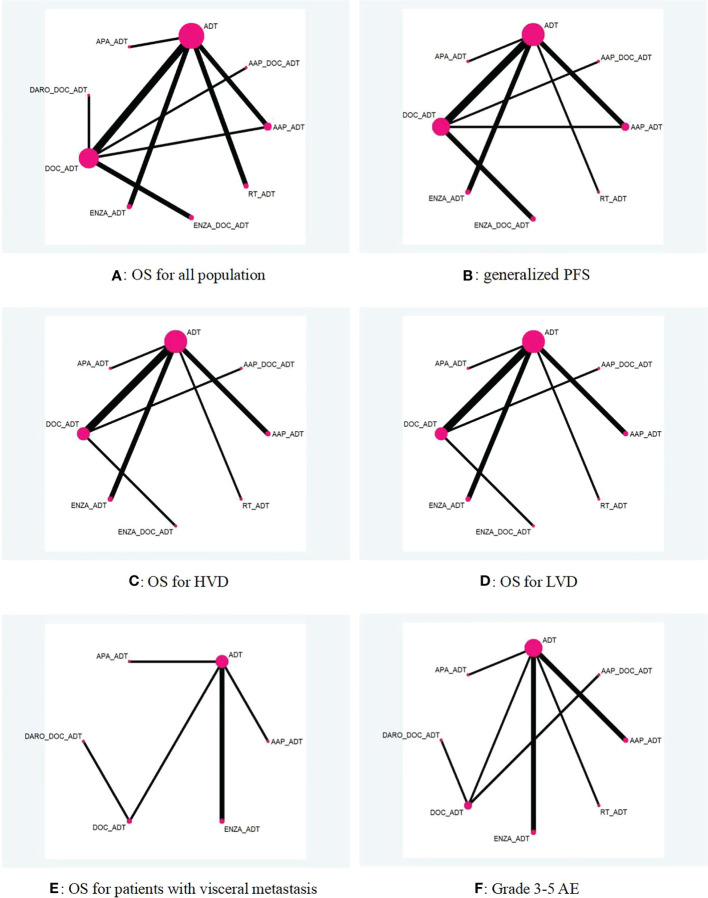
Medline, Embase, Cochrane Central and ClinicalTrials.gov were searched from inception through July 01, 2022. Eligible studies were phase III randomized clinical trials evaluating androgen deprivation treatment (ADT) alone, doublet therapies [ADT combined with docetaxel (DOC), novel hormonal agents (NHAs), or radiotherapy (RT)], or triplet therapies (NHA+DOC+ADT) as first-line treatments for mHSPC. Outcomes of interest included overall survival (OS), progression-free survival (PFS) and grades 3-5 adverse events (AEs). Subgroup analyses were performed based on tumor burden. The effects of competing treatments were assessed by Bayesian network meta-analysis using R software.
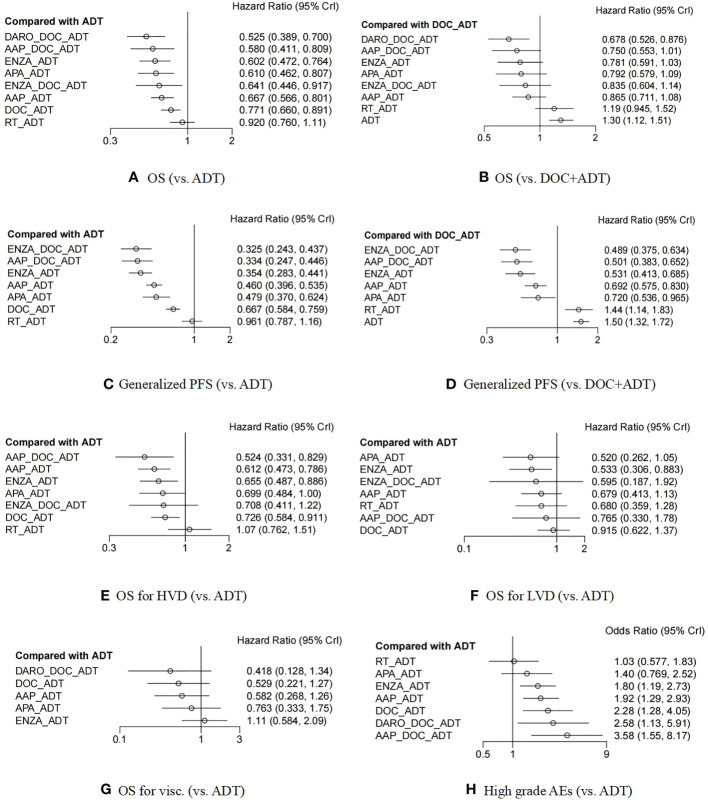
Ten trials with 12,298 patients comparing nine treatments were included. Darolutamide (DARO) +DOC+ADT ranked best in terms of OS benefits (OR 0·52 [95% CI 0·39-0·70]), but its advantages were all statistically insignificant compared with other therapy options except for DOC+ADT (OR 0·68 [95% CI 0·53-0·88]) and RT+ADT (OR 0·57 [95% CI 0·40-0·80]). In terms of PFS, enzalutamide(ENZA)+DOC+ADT (OR 0·32 [95% CI 0·24-0·44]) and abiraterone and prednisone (AAP) +DOC+ADT (OR 0·33 [95% CI 0·25-0·45]) ranked best. For patients with high volume disease (HVD), low volume disease (LVD), and visceral metastases, the optimal therapies were AAP+DOC+ADT (OR 0·52 [95% CI 0·33-0·83]), apalutamide+ADT (OR 0·52 [95% CI 0·26-1·05]) and DARO+DOC+ADT (OR 0·42 [95% CI 0·13-1·34]), respectively. For safety, AAP+DOC+ADT (OR 3·56 [95% CI 1·51-8·43]) ranked worst with the highest risk of grade 3-5 AEs.
Triple therapies may further improve OS and PFS but may be associated with a decrease in safety. Triplet therapies could be suggested for HVD patients, while doublet combinations should still be preferred for LVD patients.
https://www.crd.york.ac.uk/PROSPEROFILES/303117_STRATEGY_20220202.pdf, identifier CRD4202303117.
转移性激素敏感性前列腺癌(mHSPC)一线治疗的最佳选择尚不清楚。我们旨在比较mHSPC双联和三联治疗的随机临床试验中确定的有效性和安全性。
检索Medline、Embase、Cochrane Central和ClinicalTrials.gov,检索时间从数据库创建至2022年7月1日。符合条件的研究为III期随机临床试验,评估单独雄激素剥夺治疗(ADT)、双联疗法[ADT联合多西他赛(DOC)、新型激素药物(NHA)或放疗(RT)]或三联疗法(NHA+DOC+ADT)作为mHSPC的一线治疗。感兴趣的结局包括总生存期(OS)、无进展生存期(PFS)和3-5级不良事件(AE)。基于肿瘤负荷进行亚组分析。使用R软件通过贝叶斯网络荟萃分析评估竞争性治疗的效果。
纳入了10项试验,共12298例患者,比较了9种治疗方法。达罗他胺(DARO)+DOC+ADT在OS获益方面排名最佳(比值比0.52[95%置信区间0.39-0.70]),但其优势与除DOC+ADT(比值比0.68[95%置信区间0.53-0.88])和RT+ADT(比值比0.57[95%置信区间0.40-0.80])之外的其他治疗方案相比,均无统计学意义。在PFS方面,恩杂鲁胺(ENZA)+DOC+ADT(比值比0.32[95%置信区间0.24-0.44])和阿比特龙和泼尼松(AAP)+DOC+ADT(比值比0.33[95%置信区间0.25-0.45])排名最佳。对于高肿瘤负荷疾病(HVD)、低肿瘤负荷疾病(LVD)和内脏转移患者,最佳治疗方案分别为AAP+DOC+ADT(比值比0.52[95%置信区间0.33-0.83])、阿帕他胺+ADT(比值比0.52[95%置信区间0.26-1.05])和DARO+DOC+ADT(比值比0.42[95%置信区间0.13-1.34])。在安全性方面,AAP+DOC+ADT(比值比3.56[95%置信区间1.51-8.43])排名最差,3-5级AE风险最高。
三联疗法可能进一步改善OS和PFS,但可能与安全性下降有关。对于HVD患者可建议采用三联疗法,而LVD患者仍应首选双联组合疗法。
https://www.crd.york.ac.uk/PROSPEROFILES/303117_STRATEGY_20220202.pdf,标识符CRD4202303117。