Franovic Sreten, Pietroski Alexander D, Druskovich Katherine, Page Brendan, Burdick Gabriel B, Fathima Bushra, McIntosh Michael J, King Elizabeth A, Muh Stephanie J
Department of Orthopaedic Surgery, Henry Ford Health System, Detroit, MI.
J Hand Surg Glob Online. 2022 Dec 28;5(2):169-177. doi: 10.1016/j.jhsg.2022.11.007. eCollection 2023 Mar.
To conduct a cost-effectiveness study of nonsurgical and surgical treatment options for distal radius fractures using distinct posttreatment outcome patterns.
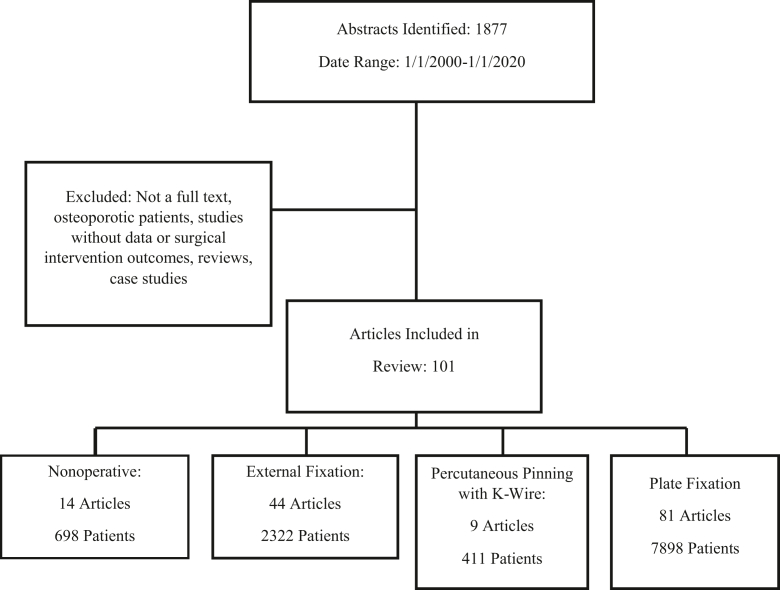
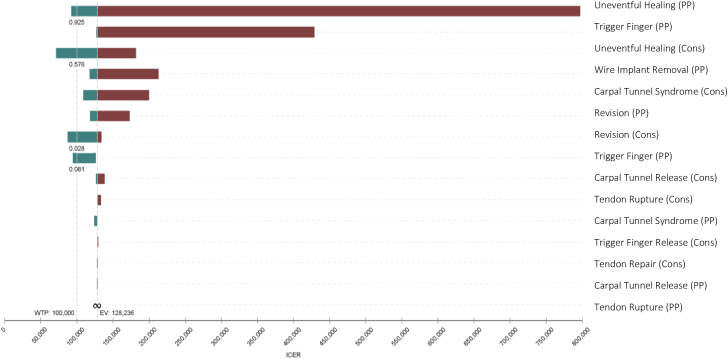
We created a decision tree to model the following treatment modalities for distal radius fractures: nonsurgical management, external fixation, percutaneous pinning, and plate fixation. Each node of the model was associated with specific costs in dollars, a utility adjustment (quality-adjusted life year [QALY]), and a percent likelihood. The nodes of the decision tree included uneventful healing, eventful healing and no further intervention, carpal tunnel syndrome, trigger finger, and tendon rupture as well as associated treatments for each event. The percent probabilities of each transition state, QALY values, and costs of intervention were gleaned from a systematic review. Rollback and incremental cost-effectiveness ratio analyses were conducted to identify optimal treatment strategies. Threshold values of $50,000/QALY and $100,000/QALY were used to distinguish the modalities in the incremental cost-effectiveness ratio analysis.
Both the rollback analysis and the incremental cost-effectiveness ratio analysis revealed nonsurgical management as the predominant strategy when compared with the other operative modalities. Nonsurgical management dominated external fixation and plate fixation, although it was comparable with percutaneous fixation, yielding a $2,242 lesser cost and 0.017 lesser effectiveness.
The cost effectiveness of nonsurgical management is driven by its decreased cost to the health care system. Plate and external fixation have been shown to be both more expensive and less effective than other proposed treatments. Percutaneous pinning has demonstrated more favorable effectiveness in the literature than plate and external fixation and, thus, may be more cost effective in certain circumstances. Future studies may find value in investigating further clinical aspects of distal radius fractures and their association with nonsurgical management versus that with plate fixation.
TYPE OF STUDY/LEVEL OF EVIDENCE: Economic/decision analysis II.
利用不同的治疗后结果模式,对桡骨远端骨折的非手术和手术治疗方案进行成本效益研究。
我们创建了一个决策树,以模拟桡骨远端骨折的以下治疗方式:非手术治疗、外固定、经皮穿针固定和钢板固定。该模型的每个节点都与以美元为单位的特定成本、效用调整值(质量调整生命年[QALY])以及百分比可能性相关联。决策树的节点包括顺利愈合、愈合过程复杂且无需进一步干预、腕管综合征、扳机指和肌腱断裂以及针对每个事件的相关治疗。每个过渡状态的百分比概率、QALY值和干预成本均来自系统评价。进行回退分析和增量成本效益比分析,以确定最佳治疗策略。在增量成本效益比分析中,使用50,000美元/QALY和100,000美元/QALY的阈值来区分不同的治疗方式。
与其他手术方式相比,回退分析和增量成本效益比分析均显示非手术治疗是主要策略。非手术治疗优于外固定和钢板固定,尽管与经皮固定相当,成本降低了2242美元,效果降低了0.017。
非手术治疗的成本效益源于其降低了医疗系统的成本。钢板和外固定已被证明比其他建议的治疗方法更昂贵且效果更差。经皮穿针固定在文献中显示出比钢板和外固定更有利的效果,因此在某些情况下可能更具成本效益。未来的研究可能会发现,进一步研究桡骨远端骨折的临床方面及其与非手术治疗和钢板固定的关联具有价值。
研究类型/证据水平:经济/决策分析II级。