Chang Chia-Yau, Chiou Shyh-Shin, Weng Te-Fu, Lin Pei-Chin, Lai Shiue-Wei, Tsai Chen-Hua, Liu Yen-Lin, Ku Jung-Tzu, Liao Yu-Mei, Tsai Jia-Ruey, Hu Shu-Hsia, Cheng Chao-Neng, Chen Yeu-Chin
Department of Pediatrics, School of Medicine, College of Medicine, Taipei Medical University, Taipei 110, Taiwan.
Division of Pediatric Hematology/Oncology, Department of Pediatrics, Taipei Medical University Hospital, Taipei 110, Taiwan.
J Clin Med. 2023 Mar 13;12(6):2207. doi: 10.3390/jcm12062207.
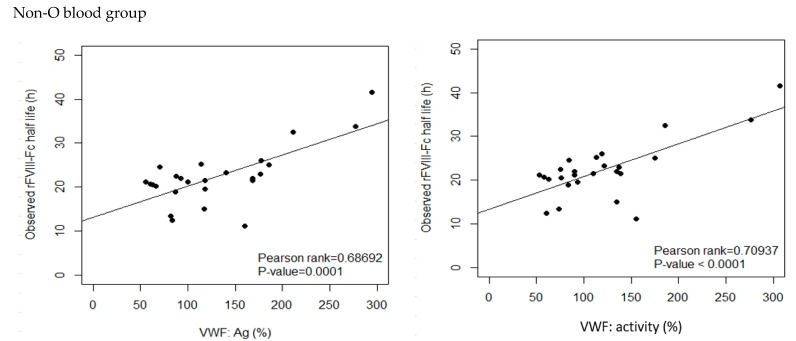
The half life of recombinant factor VIII-Fc (rFVIII-Fc) for people with hemophilia A (PwHA) varies greatly. Understanding the factors influencing the variation and assessment of rFVIII-Fc half life is important for personalized treatment. Eighty-five severe-type PwHA with rFVIII-Fc treatment receiving an evaluation of half life by the Web-Accessible Population Pharmacokinetic (PK) Service-Hemophilia during 2019-2021 were retrospectively enrolled. The 50-patient PK profiles before 2021 were used for analysis and developing prediction models of half life, and the 35-patient PK profiles in 2021 were used for external validation. The patients in the development cohort were aged 8-64, with a median rFVIII-Fc half life of 20.75 h (range, 8.25-41.5 h). By multivariate linear regression analysis, we found two, four, and five predictors of rFVIII-Fc half life for the blood groups non-O, O patients, and overall patients, respectively, including baseline VWF:Ag, BMI, VWF:activity/VWF:Ag ratio, body weight, O blood group, inhibitor history, HCV infection, and hematocrit. The three prediction equations of rFVIII-Fc half life (T) were respectively developed as T for non-O group patients = -0.81 + 0.63 × (BMI, kg/m) + 6.07 × (baseline VWF:Ag, IU/mL), T for O group patients = -0.68 + 13.30 × (baseline VWF:Ag, IU/mL) + 0.27 × (BW, kg) - 1.17 × (BMI, kg/m) + 16.02 × (VWF:activity/VWF:Ag ratio), and T for overall patients = -1.76 + 7.24 × (baseline VWF:Ag, IU/mL) - 3.84 × (Inhibitor history) + 2.99 × (HCV infection) - 2.83 × (O blood group) + 0.30 × (Hct, %), which explained 51.97%, 75.17%, and 66.38% of the half life variability, respectively. For external validation, there was a significant correlation between the predicted and observed half lives in the validation cohort. The median half life deviation was +1.53 h, +1.28 h, and +1.79 h for the equations of non-O group, O group, and overall group patients, respectively. In total, eight predictors influencing rFVIII-Fc half life were identified. Prediction equations of rFVIII-Fc half life were developed for the non-O and O blood groups and overall PwHA with a good degree of external validation. The equations could be applied to patients aged 8-64 without the need for PK blood sampling and clinically valuable for personalized therapy.
重组因子VIII-Fc(rFVIII-Fc)在A型血友病患者(PwHA)中的半衰期差异很大。了解影响rFVIII-Fc半衰期变化的因素并对其进行评估,对于个性化治疗至关重要。对2019年至2021年期间接受网络可及群体药代动力学(PK)服务-血友病评估rFVIII-Fc半衰期的85例重度A型血友病患者进行回顾性纳入。将2021年之前50例患者的PK数据用于分析并建立半衰期预测模型,2021年35例患者的PK数据用于外部验证。开发队列中的患者年龄为8至64岁,rFVIII-Fc半衰期中位数为20.75小时(范围8.25至41.5小时)。通过多变量线性回归分析,我们分别发现非O血型、O血型患者及所有患者rFVIII-Fc半衰期的两个、四个和五个预测因素,包括基线血管性血友病因子抗原(VWF:Ag)、体重指数(BMI)、血管性血友病因子活性/血管性血友病因子抗原比值(VWF:activity/VWF:Ag ratio)、体重、O血型、抑制物病史、丙型肝炎病毒(HCV)感染及血细胞比容。分别建立了rFVIII-Fc半衰期(T)的三个预测方程,非O组患者的方程为T = -0.81 + 0.63×(BMI,kg/m²)+ 6.07×(基线VWF:Ag,IU/mL),O组患者的方程为T = -0.68 + 13.30×(基线VWF:Ag,IU/mL)+ 0.27×(体重,kg) - 1.17×(BMI,kg/m²)+ 16.02×(VWF:activity/VWF:Ag ratio),所有患者的方程为T = -1.76 + 7.24×(基线VWF:Ag,IU/mL) - 3.84×(抑制物病史)+ 2.99×(HCV感染) - 2.83×(O血型)+ 0.30×(血细胞比容,%),分别解释了半衰期变异性的51.97%、75.17%和66.38%。对于外部验证,验证队列中预测半衰期与观察到的半衰期之间存在显著相关性。非O组、O组和所有组患者方程的半衰期中位数偏差分别为+1.53小时、+1.28小时和+1.79小时。总共确定了八个影响rFVIII-Fc半衰期的预测因素。为非O和O血型以及所有A型血友病患者建立了rFVIII-Fc半衰期预测方程,具有良好的外部验证度。这些方程可应用于8至64岁的患者,无需进行PK血样采集,对个性化治疗具有临床价值。