Gastroenterology and Endoscopy Unit, Fondazione IRCCS Policlinico San Matteo, 27100 Pavia, Italy.
Specialization School of Diseases of Digestive System Pavia, University of Pavia, 27100 Pavia, Italy.
Medicina (Kaunas). 2023 Mar 22;59(3):636. doi: 10.3390/medicina59030636.
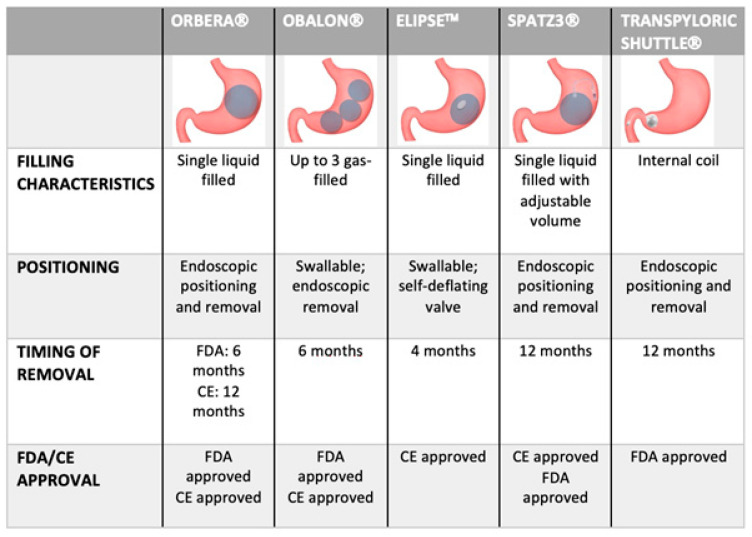
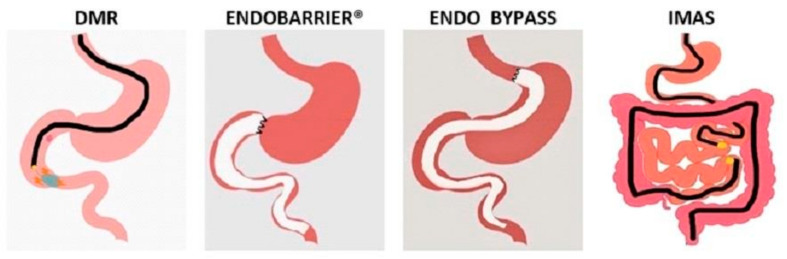
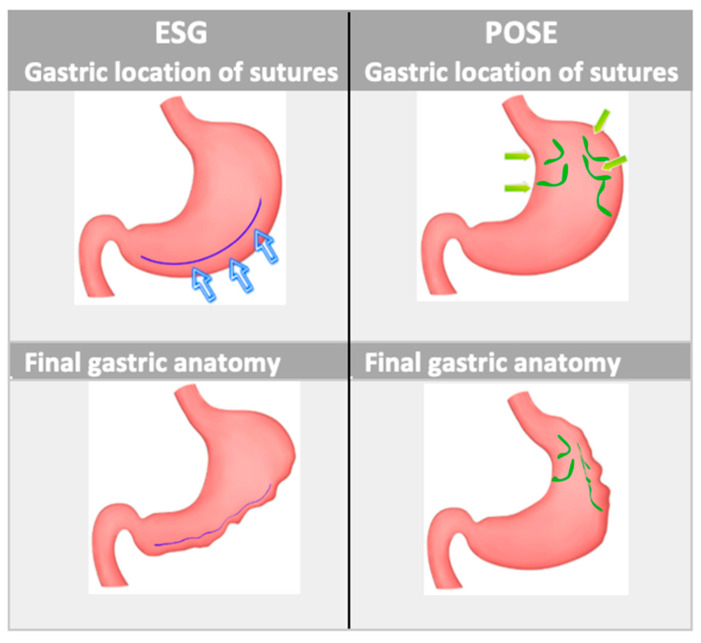
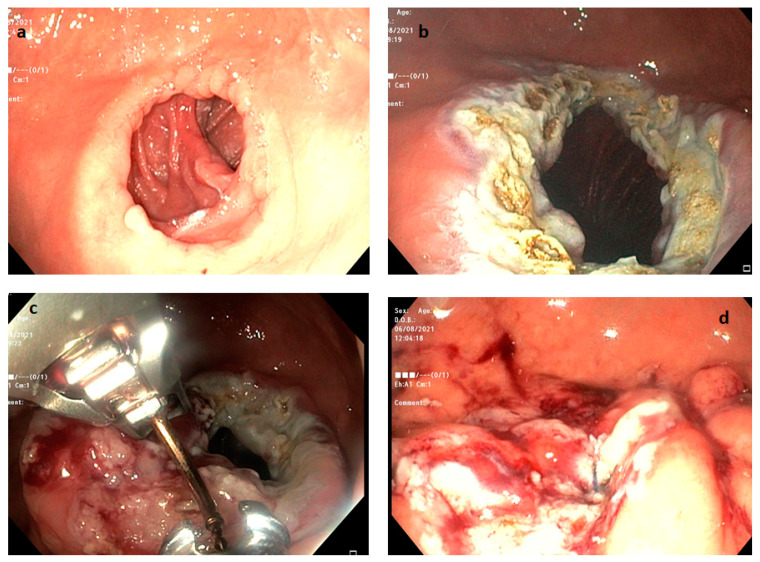
Obesity is a chronic disease that impairs quality of life and leads to several comorbidities. When conservative therapies fail, bariatric surgical options such as Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG) are the most effective therapies to induce persistent weight loss. Over the last two decades, bariatric endoscopy has become a valid alternative to surgery in specific settings. Restrictive gastric procedures, such as intragastric balloons (IGBs) and endoscopic gastroplasty, have been shown to be effective in inducing weight loss compared to diet modifications alone. Endoscopic gastroplasty is usually superior to IGBs in maintaining weight loss in the long-term period, whereas IGBs have an established role as a bridge-to-surgery approach in severely obese patients. IGBs in a minority of patients could be poorly tolerated and require early removal. More recently, novel endoscopic systems have been developed with the combined purpose of inducing weight loss and improving metabolic conditions. Duodenal mucosal resurfacing demonstrated efficacy in this field in its early trials: significant reduction from baseline of HbA1c values and a modest reduction of body weight were observed. Other endoscopic malabsorptive have been developed but need more evidence. For example, a pivotal trial on duodenojejunal bypasses was stopped due to the high rate of severe adverse events (hepatic abscesses). Optimization of these more recent malabsorptive endoscopic procedures could expand the plethora of bariatric patients that could be treated with the intention of improving their metabolic conditions. Weight regain may occur in up to one third of patients after bariatric surgery. Different endoscopic procedures are currently performed after both RYGB and SG in order to modulate post-surgical anatomy. The application of argon plasma coagulation associated with endoscopic full-thickness suturing systems (APC-TORe) and Re-EndoSleeve have shown to be the most effective endoscopic treatments after RYGB and SG, respectively. Both procedures are usually well tolerated and have a very low risk of stricture. However, APC-TORe may sometimes require more than one session to obtain adequate final results. The aim of this review is to explore all the currently available primary and revisional endoscopic bariatric therapies focusing on their efficacy and safety and their potential application in clinical practice.
肥胖是一种慢性疾病,会降低生活质量并导致多种合并症。当保守治疗失败时,减重手术选择,如 Roux-en-Y 胃旁路术(RYGB)和袖状胃切除术(SG),是诱导持续体重减轻的最有效治疗方法。在过去的二十年中,减重内镜已成为特定情况下手术的有效替代方法。与单纯饮食改变相比,限制型胃手术,如胃内球囊(IGB)和内镜胃成形术,已被证明能有效诱导体重减轻。在长期期间,内镜胃成形术通常优于 IGB,而 IGB 在肥胖患者中作为手术桥接方法具有既定作用。少数患者可能无法耐受 IGB,并需要早期取出。最近,开发了新的内镜系统,其共同目的是诱导体重减轻和改善代谢状况。十二指肠黏膜再表面处理在早期试验中显示出在该领域的疗效:从基线观察到 HbA1c 值显著降低和体重适度减轻。其他内镜吸收不良也已开发出来,但需要更多证据。例如,由于严重不良事件(肝脓肿)的发生率高,十二指肠空肠旁路的关键试验被停止。这些最近的吸收不良内镜手术的优化可以扩大可以治疗的肥胖患者的数量,以改善他们的代谢状况。减重手术后,多达三分之一的患者可能会出现体重反弹。目前,在 RYGB 和 SG 之后,为了调节手术后的解剖结构,会进行不同的内镜程序。氩等离子凝固联合内镜全层缝合系统(APC-TORe)和 Re-EndoSleeve 的应用已被证明分别是 RYGB 和 SG 后最有效的内镜治疗方法。这两种程序通常都能很好地耐受,并且狭窄的风险非常低。然而,APC-TORe 有时可能需要不止一次治疗才能获得足够的最终结果。本综述的目的是探讨所有现有的原发性和复发性内镜减重治疗方法,重点关注其疗效和安全性,以及它们在临床实践中的潜在应用。